Swami Umang, Sinnott Jennifer Anne, Haaland Benjamin, Sayegh Nicolas, McFarland Taylor Ryan, Tripathi Nishita, Maughan Benjamin L, Rathi Nityam, Sirohi Deepika, Nussenzveig Roberto, Kohli Manish, Pal Sumanta K, Agarwal Neeraj
Division of Oncology, Department of Internal Medicine, Huntsman Cancer Institute, University of Utah, Salt Lake City, UT 84112, USA.
Department of Internal Medicine, University of Utah, Salt Lake City, UT 84132, USA.
Cancers (Basel). 2021 Sep 30;13(19):4951. doi: 10.3390/cancers13194951.
Both novel hormonal therapies and docetaxel are approved for treatment of metastatic prostate cancer (mPC; in castration sensitive or refractory settings). Present knowledge gaps include lack of real-world data on treatment patterns in patients with newly diagnosed mPC, and comparative effectiveness of novel hormonal therapies (NHT) versus docetaxel after treatment with a prior NHT.
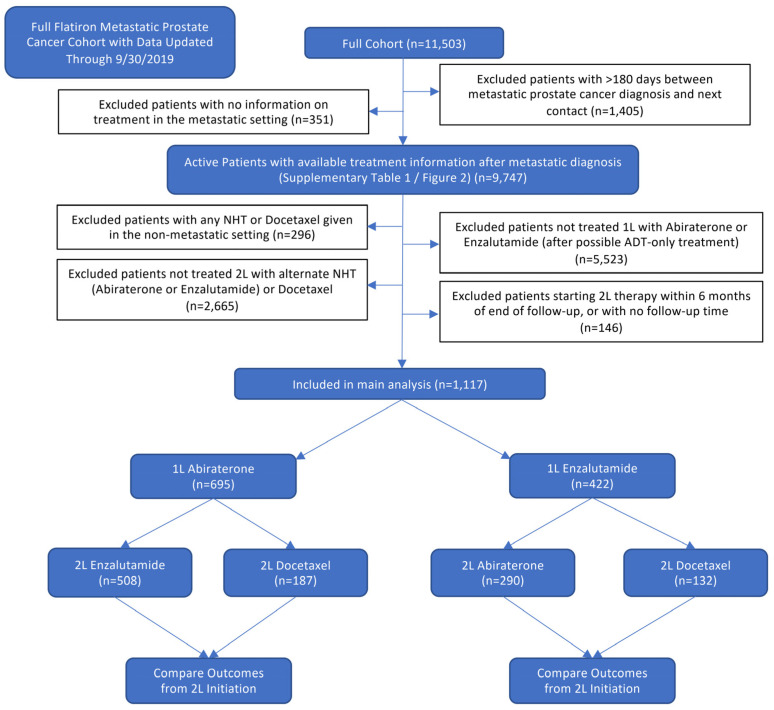
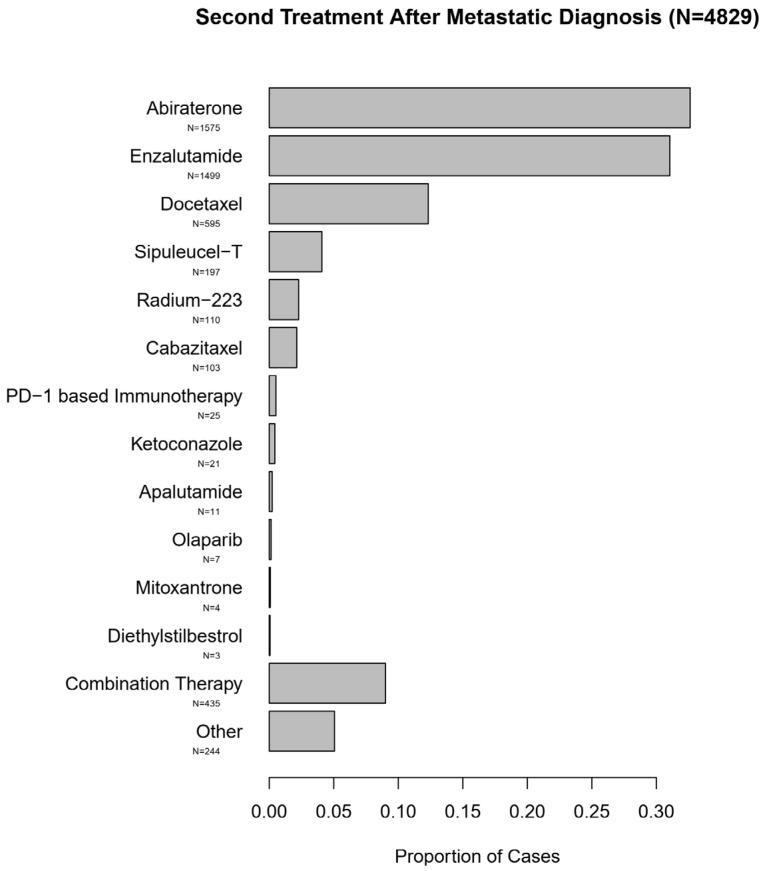
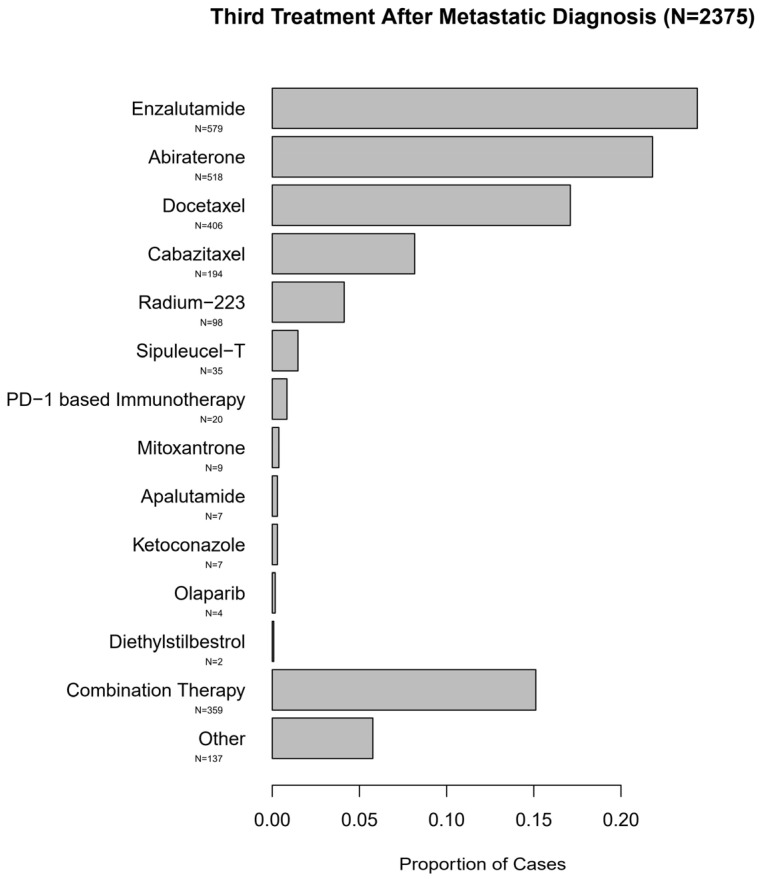
Herein we extracted patient-level data from a large real-world database of patients with mPC in United States. Utilization of NHT or docetaxel for mPC and comparative effectiveness of an alternate NHT versus docetaxel after one prior NHT was evaluated. Comparative effectiveness was examined via Cox proportional hazards model with propensity score matching weights. Each patient's propensity for treatment was modeled via random forest based on 22 factors potentially driving treatment selection.
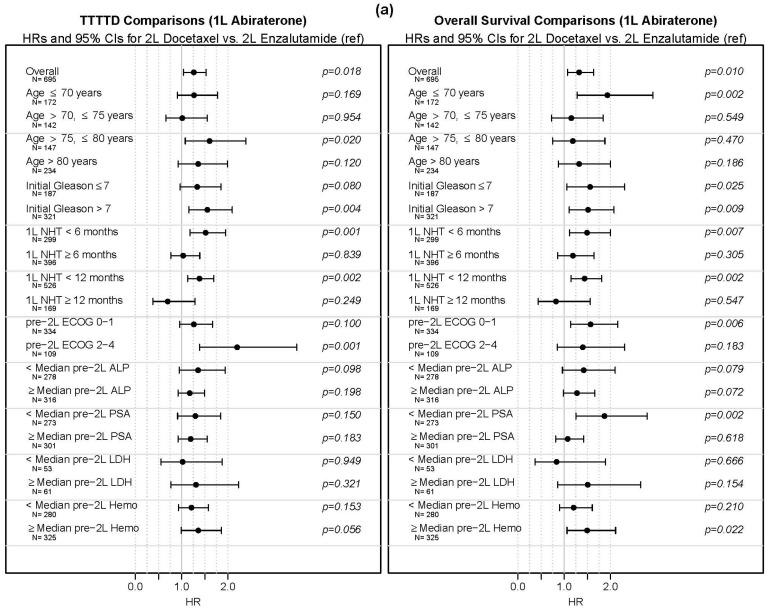
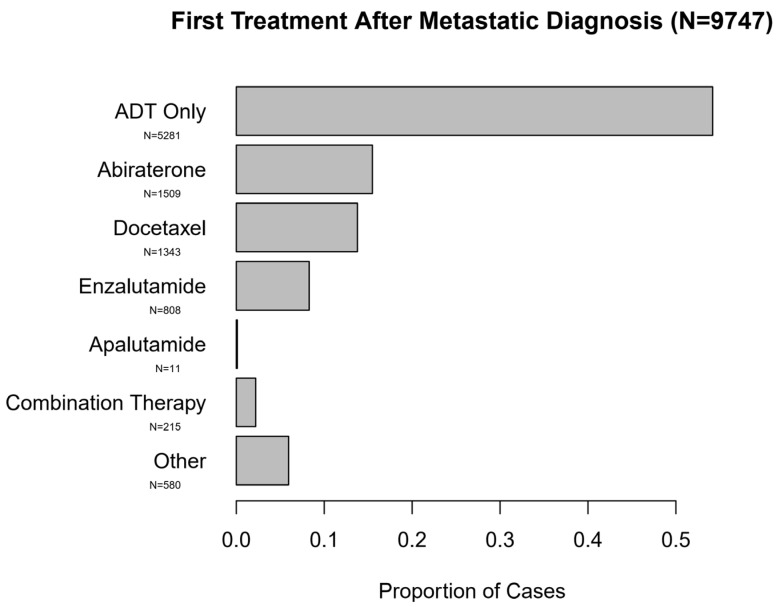
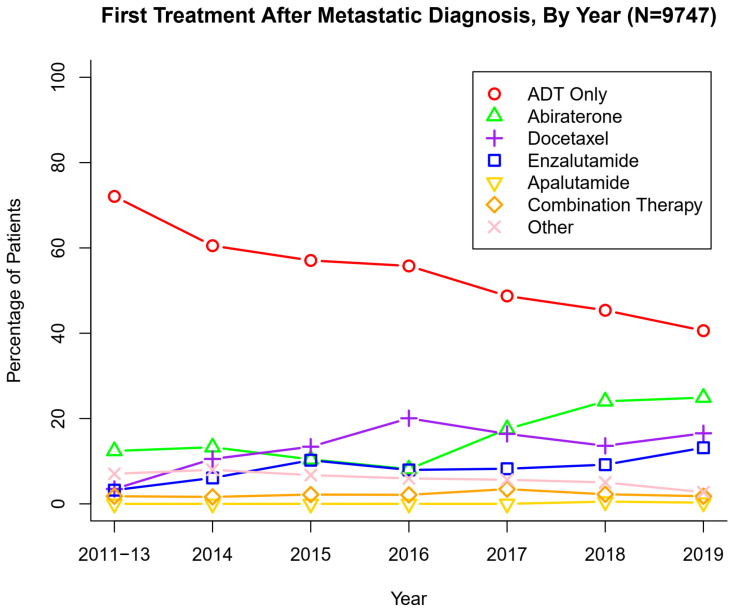
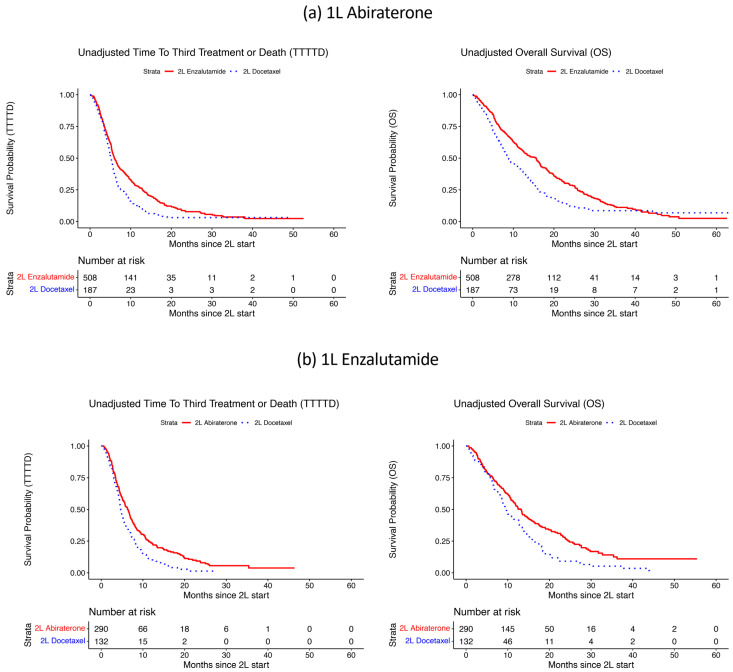
The majority of patients (54%) received only androgen deprivation therapy for mPC. In patients treated with an NHT, alternate NHT was the most common next therapy and was associated with improved median overall survival over docetaxel (abiraterone followed by docetaxel vs. enzalutamide (8.7 vs. 15.6 months; adjusted hazards ratio; aHR 1.32; = 0.009; and enzalutamide followed by docetaxel vs. abiraterone (9.7 vs. 13.2 months aHR 1.40; = 0.009). Limitations of the study include retrospective design.
新型激素疗法和多西他赛均被批准用于治疗转移性前列腺癌(mPC;去势敏感或难治性情况下)。目前的知识空白包括缺乏新诊断mPC患者治疗模式的真实世界数据,以及新型激素疗法(NHT)与在接受过一次NHT治疗后使用多西他赛的比较疗效。
在此,我们从美国一个大型mPC患者真实世界数据库中提取了患者层面的数据。评估了NHT或多西他赛用于mPC的情况,以及在接受过一次NHT后,另一种NHT与多西他赛的比较疗效。通过具有倾向评分匹配权重的Cox比例风险模型检查比较疗效。基于22个可能驱动治疗选择的因素,通过随机森林对每位患者的治疗倾向进行建模。
大多数患者(54%)仅接受了mPC的雄激素剥夺治疗。在接受NHT治疗的患者中,另一种NHT是最常见的后续治疗,与多西他赛相比,其总生存期中位数有所改善(阿比特龙序贯多西他赛与恩杂鲁胺相比,分别为8.7个月和15.6个月;调整后风险比;aHR 1.32;P = 0.009;恩杂鲁胺序贯多西他赛与阿比特龙相比,分别为9.7个月和13.2个月,aHR 1.40;P = 0.009)。该研究的局限性包括回顾性设计。