George Mathew, Smith Alexandra, Sabesan Sabe, Ranmuthugala Geetha
North West Cancer Centre, Tamworth Hospital, Hunter New England Local Health District, Tamworth, Australia.
School of Rural Medicine, University of New England, Armidale, Australia.
JMIR Cancer. 2021 Oct 13;7(4):e26425. doi: 10.2196/26425.
Cancer is one of the predominant causes of morbidity and mortality in older adult populations worldwide. Among a range of barriers, comorbidity particularly poses a clinical challenge in cancer diagnosis, prognosis, and treatment owing to its heterogeneous nature. While accurate comorbidity assessments and appropriate treatment administration can result in better patient outcomes, evidence related to older adult cancer populations is limited as these individuals are often excluded from regular clinical trials due to age and comorbid conditions.
To determine the prevalence of physical comorbidity and the impact of physical comorbidities and rurality on treatment and its outcomes in older adult cancer populations.
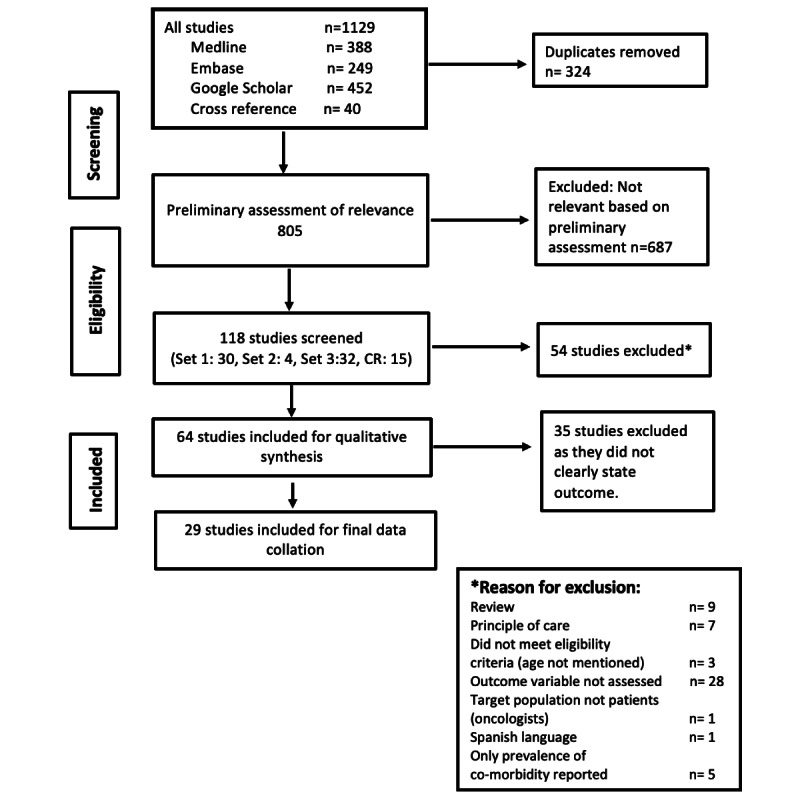
Scientific databases Embase and PubMed were searched for published scientific literature on physical comorbidity and older adult cancer patients. Google Scholar was searched for scholarly literature published in nonindexed journals. Snowballing was utilized to identify research papers missed in the above searches. Included studies : (1) reported on original research involving cancer patients; (2) included patients aged 65 years or older; (3) had patients receiving cancer-related treatment and (4) cancer survivors; (5) reported on physical comorbidity as a variable; (6) were published in English; and (7) conducted from any geographical location.
In total, 29 studies were selected for data extraction, evidence synthesis, and quality assessment. In these, comorbidities ranged from 37.9%-74.3% in colorectal cancer, 74%-81% in head and neck cancer, and 12.6%-49% in breast cancer. Moderate comorbidities ranged from 13%-72.9%, and severe comorbidities from 2.5%-68.2%. Comorbidity increased with age, with comorbidity affecting both treatment choice and process. Physical comorbidities significantly affected treatment initiation, causing delay, toxicity, and discontinuation. Older adult cancer patients were given less vigorous and nonstandard treatments and were also less likely to be offered treatment. Where patients are given more vigorous treatment, several studies showed better survival outcomes. Appropriate treatment in older adult cancer patients increased both overall and disease-related survival rates. None of the studies noted rurality as a distinct variable.
This systematic review concludes that there is evidence to substantiate the adverse effect of comorbidity on treatment and survival outcomes. However, the mechanism by which comorbidity impedes or impacts treatment is unknown in many cases. Some low-quality evidence is available for considering the functional status and biological age in treatment decisions. Future studies that substantiate the value of comprehensive older adult assessments before treatment initiation in cancer patients, including assessing the nature and severity of comorbidities, and additional consideration of rurality as a factor, could lessen the effect of comorbidities on the treatment process.
癌症是全球老年人群发病和死亡的主要原因之一。在一系列障碍中,合并症因其异质性,在癌症诊断、预后和治疗方面尤其带来了临床挑战。虽然准确的合并症评估和适当的治疗管理可带来更好的患者预后,但与老年癌症患者群体相关的证据有限,因为这些个体常因年龄和合并症被排除在常规临床试验之外。
确定老年癌症患者群体中身体合并症的患病率,以及身体合并症和农村地区对治疗及其结果的影响。
在科学数据库Embase和PubMed中检索关于身体合并症和老年癌症患者的已发表科学文献。在谷歌学术中检索非索引期刊上发表的学术文献。采用滚雪球法识别上述检索中遗漏的研究论文。纳入研究:(1) 报告涉及癌症患者的原始研究;(2) 纳入65岁及以上患者;(3) 患者接受癌症相关治疗且 (4) 为癌症幸存者;(5) 将身体合并症作为变量进行报告;(6) 以英文发表;(7) 在任何地理位置开展。
共选择29项研究进行数据提取、证据综合和质量评估。其中,结直肠癌的合并症发生率在37.9%-74.3%之间,头颈癌为74%-81%之间,乳腺癌为12.6%-49%之间。中度合并症发生率在13%-72.9%之间,重度合并症在2.5%-68.2%之间。合并症随年龄增加而增加,合并症影响治疗选择和治疗过程。身体合并症显著影响治疗开始,导致延迟、毒性反应和治疗中断。老年癌症患者接受的积极治疗和标准化治疗较少,接受治疗的可能性也较低。在给予患者更积极治疗的情况下,多项研究显示生存结局更好。老年癌症患者的适当治疗可提高总生存率和疾病相关生存率。没有研究将农村地区作为一个显著变量。
本系统评价得出结论,有证据证实合并症对治疗和生存结果有不利影响。然而,在许多情况下,合并症阻碍或影响治疗的机制尚不清楚。有一些低质量证据可用于在治疗决策中考虑功能状态和生物学年龄。未来的研究若能证实癌症患者在开始治疗前进行全面老年评估的价值,包括评估合并症的性质和严重程度,并将农村地区作为一个因素加以额外考虑,可能会减轻合并症对治疗过程的影响。