Utsumi Masashi, Kitada Koji, Tokunaga Naoyuki, Kato Takamitsu, Narusaka Toru, Hamano Ryosuke, Miyasou Hideaki, Tsunemitsu Yousuke, Otsuka Shinya, Inagaki Masaru
Department of Surgery, National Hospital Organization Fukuyama Medical Center, 4-14-17 Okinogami-cho, Fukuyama City, Hiroshima, 720-8520, Japan.
BMC Gastroenterol. 2021 Oct 13;21(1):375. doi: 10.1186/s12876-021-01957-5.
The prognostic nutritional index, a marker of nutritional status and systemic inflammation, is a known biomarker for various cancers. However, few studies have evaluated the predictive value of the prognostic nutritional index in patients with biliary tract cancer. Therefore, we investigated the prognostic significance of the prognostic nutritional index, and developed a risk-stratification system to identify prognostic factors in patients with biliary tract cancer.
Between July 2010 and March 2021, 117 patients with biliary tract cancer were recruited to this single-center, retrospective study. The relationship between clinicopathological variables, including the prognostic nutritional index, and overall survival was analyzed using univariate and multivariate analyses. A P < 0.05 was considered statistically significant.
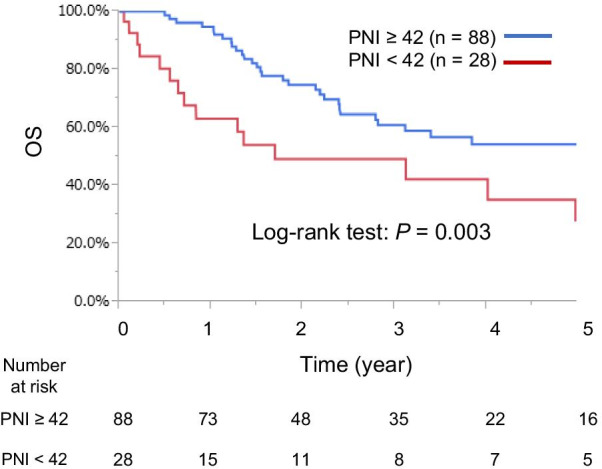
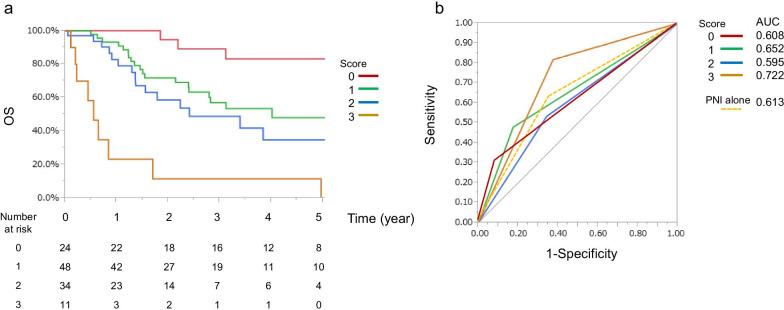
The median age was 75 (range 38-92) years. Thirty patients had intrahepatic cholangiocarcinoma; 29, gallbladder carcinoma; 27, distal cholangiocarcinoma; 17, ampullary carcinoma; and 13, perihilar cholangiocarcinoma. Curative (R0) resection was achieved in 99 patients. In univariate analysis, the prognostic nutritional index (< 42), lymph node metastasis, carbohydrate antigen 19-9 level (> 20 U/mL), preoperative cholangitis, tumor differentiation, operation time (≥ 360 min), and R1-2 resection were significant risk factors for overall survival. The prognostic nutritional index (P = 0.027), lymph node metastasis (P = 0.040), and tumor differentiation (P = 0.006) were independent prognostic factors in multivariate analysis. A combined score of the prognostic nutritional index and pathological findings outperformed each marker alone, in terms of discriminatory power.
The prognostic nutritional index, lymph node metastasis, and tumor differentiation were independent prognostic factors after surgical resection in patients with biliary tract cancer. A combined prediction model using the prognostic nutritional index and pathological findings accurately predicted prognosis, and can be used as a novel prognostic factor in patients with biliary tract cancer.
预后营养指数是营养状况和全身炎症的标志物,是多种癌症的已知生物标志物。然而,很少有研究评估预后营养指数在胆道癌患者中的预测价值。因此,我们研究了预后营养指数的预后意义,并开发了一种风险分层系统来识别胆道癌患者的预后因素。
2010年7月至2021年3月期间,117例胆道癌患者被纳入这项单中心回顾性研究。使用单因素和多因素分析来分析包括预后营养指数在内的临床病理变量与总生存期之间的关系。P < 0.05被认为具有统计学意义。
中位年龄为75岁(范围38 - 92岁)。30例为肝内胆管癌;29例为胆囊癌;27例为远端胆管癌;17例为壶腹癌;13例为肝门周围胆管癌。99例患者实现了根治性(R0)切除。在单因素分析中,预后营养指数(< 42)、淋巴结转移、糖类抗原19 - 9水平(> 20 U/mL)、术前胆管炎、肿瘤分化、手术时间(≥ 360分钟)和R1 - 2切除是总生存期的显著危险因素。在多因素分析中,预后营养指数(P = 0.027)、淋巴结转移(P = 0.040)和肿瘤分化(P = 0.006)是独立的预后因素。在鉴别能力方面,预后营养指数和病理结果的综合评分比单独的每个标志物表现更好。
预后营养指数、淋巴结转移和肿瘤分化是胆道癌患者手术切除后的独立预后因素。使用预后营养指数和病理结果的联合预测模型能够准确预测预后,并可作为胆道癌患者的一种新的预后因素。