School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town, Anzio Road, Observatory 7925, Cape Town, South Africa.
MRC Epidemiology Unit, University of Cambridge, Cambridge, UK.
AIDS Res Ther. 2021 Oct 14;18(1):72. doi: 10.1186/s12981-021-00387-3.
The growing burden of the HIV and non-communicable disease (NCD) syndemic in Sub- Saharan Africa has necessitated introduction of integrated models of care in order to leverage existing HIV care infrastructure for NCDs. However, there is paucity of literature on treatment outcomes for multimorbid patients attending integrated care. We describe 12-month treatment outcomes among multimorbid patients attending integrated antiretroviral treatment (ART) and NCD clubs in Cape Town, South Africa.
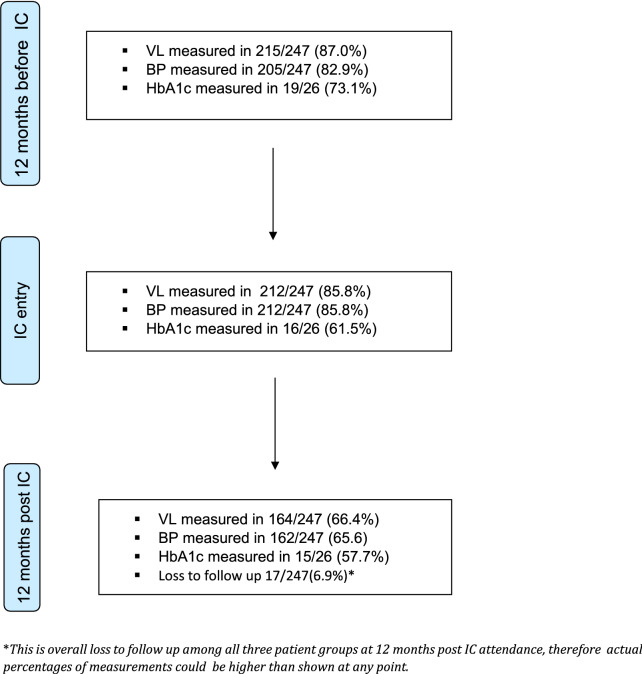
As part of an integrated clubs (IC) model pilot implemented in 2016 by the local government at two primary health care clinics in Cape Town, we identified all multimorbid patients who were enrolled for IC for at least 12 months by August 2017. Mean adherence percentages (using proxy of medication collection and attendance of club visits) and optimal disease control (defined as the proportion of participants achieving optimal blood pressure, glycosylated haemoglobin control and HIV viral load suppression where appropriate) were calculated at 12 months before, at the point of IC enrolment and 12 months after IC enrolment. Predictors of NCD control 12 months post IC enrolment were investigated using multivariable logistic regression.
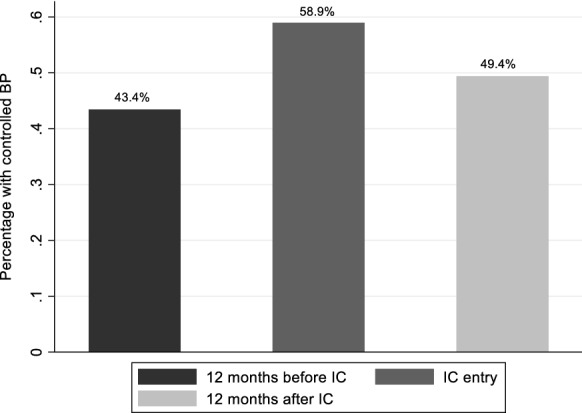
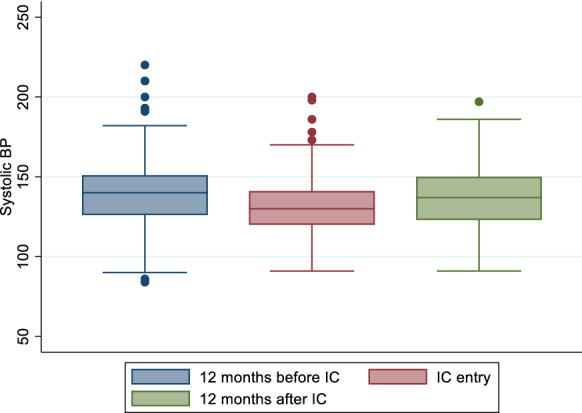
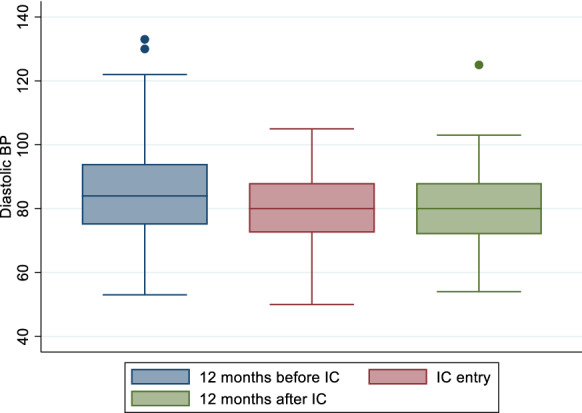
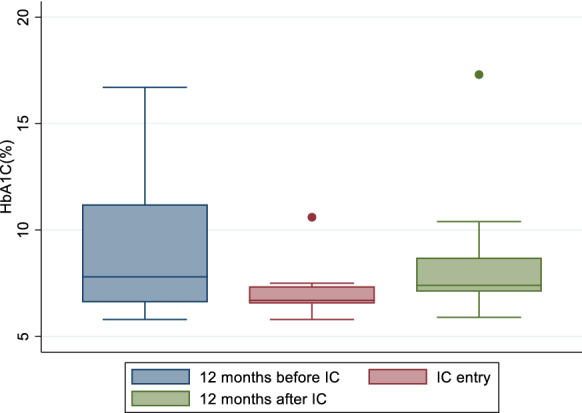
As of 31 August 2017, 247 HIV-infected patients in total had been enrolled into IC for at least 12 months. Of these, 221 (89.5%) had hypertension, 4 (1.6%) had diabetes mellitus and 22 (8.9%) had both diseases. Adherence was maintained before and after IC enrolment with mean adherence percentages of 92.2% and 94.2% respectively. HIV viral suppression rates were 98.6%, 99.5% and 99.4% at the three time points respectively. Retention in care was high with 6.9% lost to follow up at 12 months post IC enrolment. Across the 3 time-points, optimal blood pressure control was achieved in 43.1%, 58.9% and 49.4% of participants while optimal glycaemic control was achieved in 47.4%, 87.5% and 53.3% of participants with diabetes respectively. Multivariable logistic analyses showed no independent variables significantly associated with NCD control.
Multimorbid adults living with HIV achieved high levels of HIV control in integrated HIV and NCD clubs. However, intensified interventions are needed to maintain NCD control in the long term.
在撒哈拉以南非洲,艾滋病毒和非传染性疾病(NCD)的负担不断增加,这使得必须引入综合护理模式,以便利用现有的艾滋病毒护理基础设施来治疗非传染性疾病。然而,关于参加综合护理的多重疾病患者的治疗结果,文献却很少。我们描述了南非开普敦参加抗逆转录病毒治疗(ART)和非传染性疾病俱乐部的多重疾病患者的 12 个月治疗结果。
作为当地政府于 2016 年在开普敦的两个初级保健诊所实施的综合俱乐部(IC)模型试点的一部分,我们确定了所有参加 IC 至少 12 个月的多重疾病患者。在 2017 年 8 月之前、IC 登记时和登记后 12 个月,计算了 12 个月的平均依从百分比(使用药物收集和俱乐部就诊的代理)和最佳疾病控制(定义为达到最佳血压、糖化血红蛋白控制和适当的 HIV 病毒载量抑制的参与者比例)。使用多变量逻辑回归调查了 IC 登记后 12 个月 NCD 控制的预测因素。
截至 2017 年 8 月 31 日,共有 247 名 HIV 感染者总共参加了至少 12 个月的 IC。其中,221 名(89.5%)患有高血压,4 名(1.6%)患有糖尿病,22 名(8.9%)同时患有两种疾病。IC 登记前后的依从性保持不变,平均依从百分比分别为 92.2%和 94.2%。HIV 病毒抑制率分别为 98.6%、99.5%和 99.4%。在 IC 登记后 12 个月,只有 6.9%的人失去随访。在所有 3 个时间点,最佳血压控制在 43.1%、58.9%和 49.4%的参与者中得到实现,而最佳血糖控制在患有糖尿病的 47.4%、87.5%和 53.3%的参与者中得到实现。多变量逻辑分析显示,没有任何独立变量与 NCD 控制显著相关。
在综合 HIV 和 NCD 俱乐部中,患有多重疾病的艾滋病毒感染者实现了高水平的 HIV 控制。然而,需要加强干预措施,以长期维持 NCD 控制。