Department of Intensive Care and Laboratory of Experimental Intensive Care and Anaesthesiology (L·E·I·C·A), Amsterdam UMC, Amsterdam, Netherlands.
Division of Pulmonary and Critical Care Medicine, University of Michigan, Ann Arbor, MI, USA.
Lancet Respir Med. 2021 Dec;9(12):1377-1386. doi: 10.1016/S2213-2600(21)00365-9. Epub 2021 Oct 13.
Patients with COVID-19-related acute respiratory distress syndrome (ARDS) have been postulated to present with distinct respiratory subphenotypes. However, most phenotyping schema have been limited by sample size, disregard for temporal dynamics, and insufficient validation. We aimed to identify respiratory subphenotypes of COVID-19-related ARDS using unbiased data-driven approaches.
PRoVENT-COVID was an investigator-initiated, national, multicentre, prospective, observational cohort study at 22 intensive care units (ICUs) in the Netherlands. Consecutive patients who had received invasive mechanical ventilation for COVID-19 (aged 18 years or older) served as the derivation cohort, and similar patients from two ICUs in the USA served as the replication cohorts. COVID-19 was confirmed by positive RT-PCR. We used latent class analysis to identify subphenotypes using clinically available respiratory data cross-sectionally at baseline, and longitudinally using 8-hourly data from the first 4 days of invasive ventilation. We used group-based trajectory modelling to evaluate trajectories of individual variables and to facilitate potential clinical translation. The PRoVENT-COVID study is registered with ClinicalTrials.gov, NCT04346342.
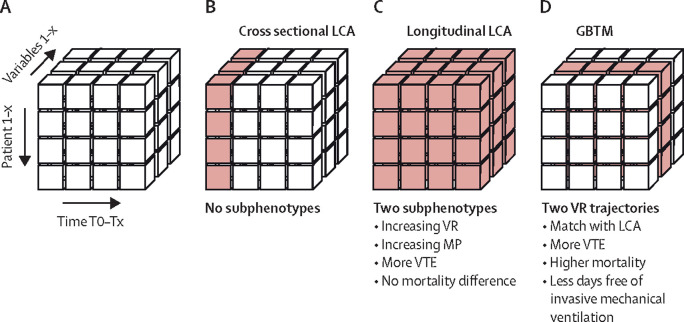
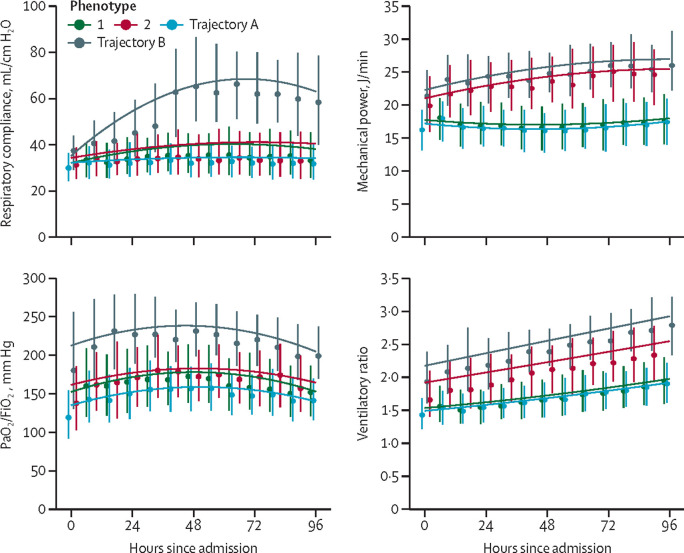
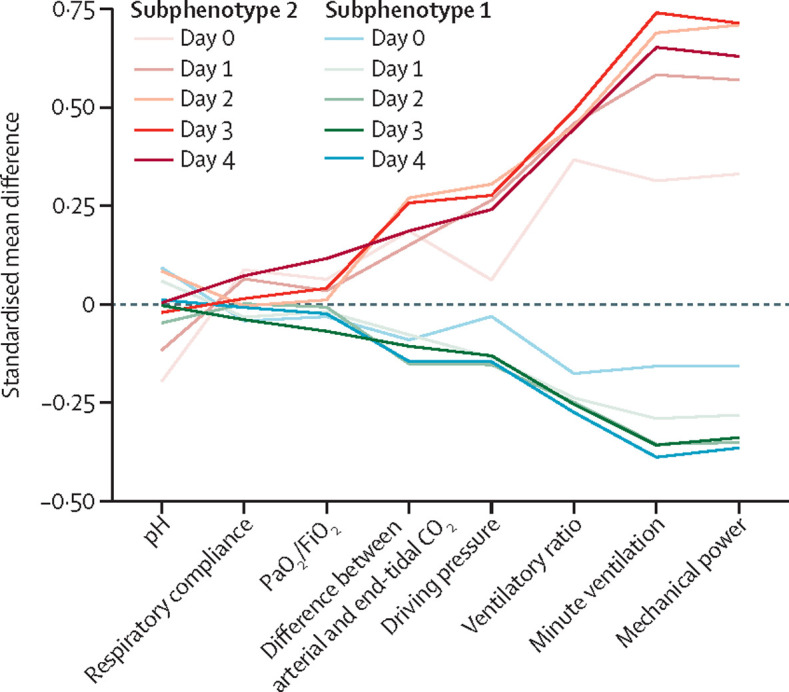
Between March 1, 2020, and May 15, 2020, 1007 patients were admitted to participating ICUs in the Netherlands, and included in the derivation cohort. Data for 288 patients were included in replication cohort 1 and 326 in replication cohort 2. Cross-sectional latent class analysis did not identify any underlying subphenotypes. Longitudinal latent class analysis identified two distinct subphenotypes. Subphenotype 2 was characterised by higher mechanical power, minute ventilation, and ventilatory ratio over the first 4 days of invasive mechanical ventilation than subphenotype 1, but PaO/FiO, pH, and compliance of the respiratory system did not differ between the two subphenotypes. 185 (28%) of 671 patients with subphenotype 1 and 109 (32%) of 336 patients with subphenotype 2 had died at day 28 (p=0·10). However, patients with subphenotype 2 had fewer ventilator-free days at day 28 (median 0, IQR 0-15 vs 5, 0-17; p=0·016) and more frequent venous thrombotic events (109 [32%] of 336 patients vs 176 [26%] of 671 patients; p=0·048) compared with subphenotype 1. Group-based trajectory modelling revealed trajectories of ventilatory ratio and mechanical power with similar dynamics to those observed in latent class analysis-derived trajectory subphenotypes. The two trajectories were: a stable value for ventilatory ratio or mechanical power over the first 4 days of invasive mechanical ventilation (trajectory A) or an upward trajectory (trajectory B). However, upward trajectories were better independent prognosticators for 28-day mortality (OR 1·64, 95% CI 1·17-2·29 for ventilatory ratio; 1·82, 1·24-2·66 for mechanical power). The association between upward ventilatory ratio trajectories (trajectory B) and 28-day mortality was confirmed in the replication cohorts (OR 4·65, 95% CI 1·87-11·6 for ventilatory ratio in replication cohort 1; 1·89, 1·05-3·37 for ventilatory ratio in replication cohort 2).
At baseline, COVID-19-related ARDS has no consistent respiratory subphenotype. Patients diverged from a fairly homogenous to a more heterogeneous population, with trajectories of ventilatory ratio and mechanical power being the most discriminatory. Modelling these parameters alone provided prognostic value for duration of mechanical ventilation and mortality.
Amsterdam UMC.
据推测,与 COVID-19 相关的急性呼吸窘迫综合征(ARDS)患者存在不同的呼吸亚表型。然而,大多数表型方案受到样本量、忽视时间动态和验证不足的限制。我们旨在使用无偏倚的数据驱动方法来识别与 COVID-19 相关的 ARDS 的呼吸亚表型。
PROVENT-COVID 是一项由阿姆斯特丹大学医学中心发起的、全国性的、多中心的、前瞻性的、观察性队列研究,在荷兰的 22 个重症监护病房(ICU)进行。连续接受有创机械通气治疗的 COVID-19 患者(年龄 18 岁或以上)作为推导队列,来自美国的 2 个 ICU 的类似患者作为复制队列。通过实时逆转录聚合酶链反应(RT-PCR)确认 COVID-19。我们使用潜在类别分析(LCA),在基线时使用临床可用的呼吸数据进行横断面分析,在有创通气的前 4 天使用 8 小时的数据进行纵向分析,以识别亚表型。我们使用基于群组的轨迹建模来评估个体变量的轨迹,并促进潜在的临床转化。PROVENT-COVID 研究在 ClinicalTrials.gov 上注册,编号为 NCT04346342。
在 2020 年 3 月 1 日至 5 月 15 日期间,共有 1007 名患者入住参与的 ICU,其中 1007 名患者被纳入推导队列。复制队列 1 纳入了 288 名患者,复制队列 2 纳入了 326 名患者。横断面潜在类别分析没有发现任何潜在的亚表型。纵向潜在类别分析确定了两种不同的亚表型。亚表型 2 在有创机械通气的前 4 天内,机械功率、分钟通气量和通气比较高,而亚表型 1 的 PaO/FiO、pH 值和呼吸系统顺应性无差异。亚表型 1 组的 185 名(28%)和亚表型 2 组的 109 名(32%)患者在第 28 天死亡(p=0.10)。然而,亚表型 2 患者在第 28 天的无呼吸机天数较少(中位数 0,IQR 0-15 与 5,0-17;p=0.016),静脉血栓栓塞事件更频繁(336 名患者中有 109 名(32%)与 671 名患者中有 176 名(26%);p=0.048)。基于群组的轨迹建模揭示了通气比和机械功率的轨迹,与潜在类别分析衍生的轨迹亚表型具有相似的动态。两条轨迹分别为:通气比或机械功率在有创机械通气的前 4 天内保持稳定值(轨迹 A)或上升轨迹(轨迹 B)。然而,上升轨迹是 28 天死亡率的更好的独立预后因素(通气比为 1.64,95%CI 1.17-2.29;机械功率为 1.82,95%CI 1.24-2.66)。在复制队列中也证实了上升的通气比轨迹(轨迹 B)与 28 天死亡率之间的关联(通气比在复制队列 1 中为 4.65,95%CI 1.87-11.6;通气比在复制队列 2 中为 1.89,95%CI 1.05-3.37)。
在基线时,与 COVID-19 相关的 ARDS 没有一致的呼吸亚表型。患者从相当同质的人群转变为更异质的人群,通气比和机械功率的轨迹最具鉴别力。单独对这些参数进行建模可以为机械通气时间和死亡率提供预后价值。
阿姆斯特丹大学医学中心。