Department of Anesthesiology and Critical Care Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland.
Maryland Spine Center at Mercy, Baltimore, Maryland.
Anesthesiology. 2021 Dec 1;135(6):992-1003. doi: 10.1097/ALN.0000000000004015.
Reducing depth of anesthesia and anesthetic exposure may help prevent delirium, but trials have been conflicting. Most studies were conducted under general anesthesia or in cognitively impaired patients. It is unclear whether reducing depth of anesthesia beyond levels consistent with general anesthesia reduces delirium in cognitively intact patients. The authors' objective was to determine whether a bundled approach to reduce anesthetic agent exposure as determined by Bispectral Index (BIS) values (spinal anesthesia with targeted sedation based on BIS values) compared with general anesthesia (masked BIS) reduces delirium.
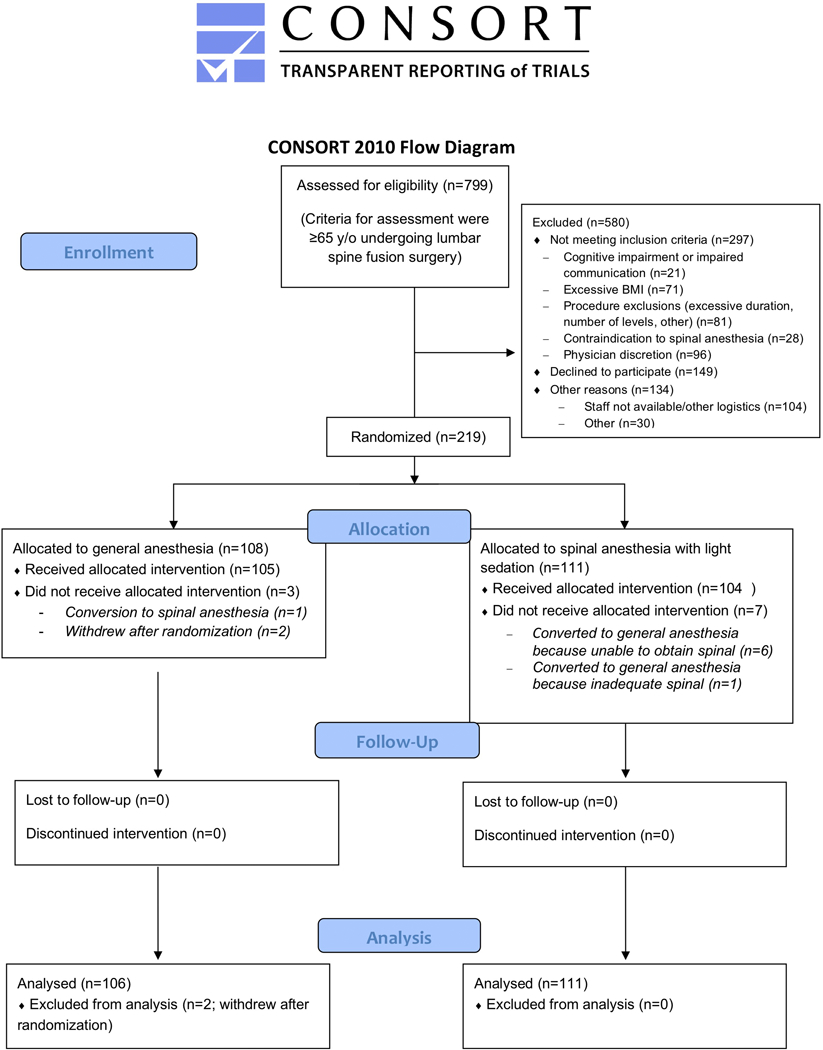
Important eligibility criteria for this parallel-arm randomized trial were patients 65 yr or greater undergoing lumbar spine fusion. The intervention group received spinal anesthesia with targeted sedation to BIS greater than 60 to 70. The control group received general anesthesia (masked BIS). The primary outcome was delirium using the Confusion Assessment Method daily through postoperative day 3, with blinded assessment.
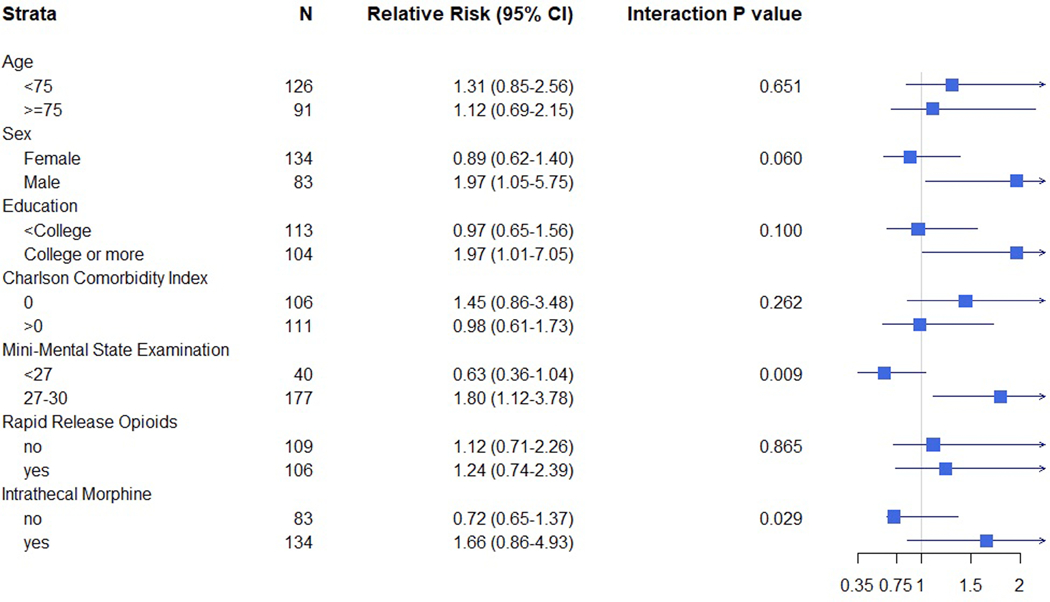
The median age of 217 patients in the analysis was 72 (interquartile range, 69 to 77). The median BIS value in the spinal anesthesia with targeted sedation based on BIS values group was 62 (interquartile range, 53 to 70) and in the general anesthesia with masked BIS values group was 45 (interquartile range, 41 to 50; P < 0.001). Incident delirium was not different in the spinal anesthesia with targeted sedation based on BIS values group (25.2% [28 of 111] vs. the general anesthesia with masked BIS values group (18.9% [20 of 106]; P = 0.259; relative risk, 1.22 [95% CI, 0.85 to 1.76]). In prespecified subgroup analyses, the effect of anesthetic strategy differed according to the Mini-Mental State Examination, but not the Charlson Comorbidity Index or age. Two strokes occurred among patients receiving spinal anesthesia and one death among patients receiving general anesthesia.
Spinal anesthesia with targeted sedation based on BIS values compared with general anesthesia with masked BIS values did not reduce delirium after lumbar fusion.
降低麻醉深度和麻醉暴露可能有助于预防谵妄,但试验结果存在冲突。大多数研究都是在全身麻醉或认知障碍患者中进行的。目前尚不清楚在全身麻醉一致的水平之外降低麻醉深度是否会减少认知完整患者的谵妄。作者的目的是确定通过脑电双频指数(BIS)值确定的麻醉药物暴露减少的综合方法(基于 BIS 值的目标镇静的脊髓麻醉)与全身麻醉(掩蔽 BIS)相比是否会降低腰椎融合术后的谵妄。
本平行臂随机试验的重要入选标准是 65 岁或以上行腰椎融合术的患者。干预组接受基于 BIS 值大于 60 至 70 的目标镇静的脊髓麻醉。对照组接受全身麻醉(掩蔽 BIS)。主要结局是术后第 3 天每天使用意识混乱评估方法进行的谵妄评估,评估采用盲法。
分析中 217 例患者的中位年龄为 72 岁(四分位距,69 至 77)。基于 BIS 值的目标镇静的脊髓麻醉组的中位 BIS 值为 62(四分位距,53 至 70),全身麻醉掩蔽 BIS 值组为 45(四分位距,41 至 50;P<0.001)。基于 BIS 值的目标镇静的脊髓麻醉组(25.2%[28/111])与全身麻醉掩蔽 BIS 值组(18.9%[20/106])的谵妄发生率无差异(P=0.259;相对风险,1.22[95%CI,0.85 至 1.76])。在预先指定的亚组分析中,麻醉策略的效果根据简易精神状态检查而不同,但与 Charlson 合并症指数或年龄无关。脊髓麻醉组发生 2 例脑卒中,全身麻醉组发生 1 例死亡。
与全身麻醉掩蔽 BIS 值相比,基于 BIS 值的目标镇静的脊髓麻醉并未降低腰椎融合术后的谵妄。