Agarwal Anurag, Rastogi Shivani, Bansal Manjari, Kumar Suraj, Malviya Deepak, Thacker Anup K
Department of Anesthesiology, CCM and Pain Medicine, Dr. RMLIMS, Lucknow, Uttar Pradesh, India.
Department of Neurology, Dr. RMLIMS, Lucknow, Uttar Pradesh, India.
Anesth Essays Res. 2021 Jan-Mar;15(1):14-19. doi: 10.4103/aer.aer_56_21. Epub 2021 Aug 30.
Idiopathic trigeminal neuralgia (TGN) is a chronic pain disorder causing unilateral, severe brief stabbing recurrent pain in the distribution of one or more branches of the trigeminal nerve. Conventional radiofrequency (CRF) and pulsed radiofrequency (PRF) are two types of minimally invasive treatment. CRF selectively ablates the part of ganglion to provide the relief, but it has been found to be associated with some side effects such as dysesthesia or sensory loss in 6%-28% and loss of corneal reflex in 3%-8% of patients. PRF is a comparatively newer modality which is a nondestructive and neuromodulatory method of delivering radiofrequency energy to the gasserian ganglion to produce a therapeutic effect.
We aimed to compare the efficacy of CRF with long-duration, fixed voltage PRF in the treatment of idiopathic TGN.
This study was conducted in a tertiary care center research institute.
This was a prospective randomized trial.
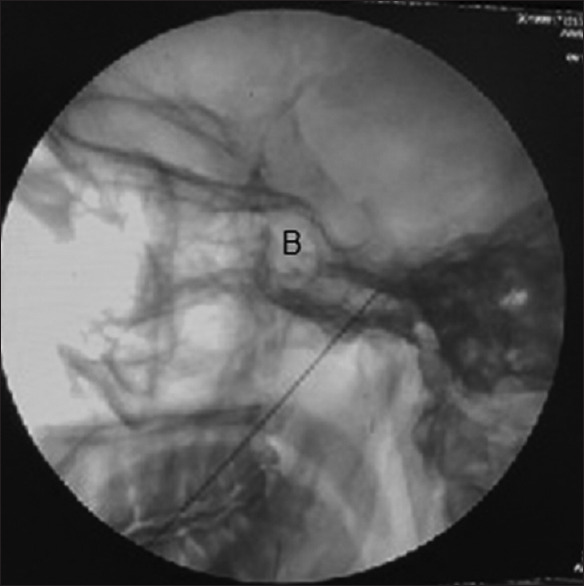
Twenty-seven adult patients of TGN were included in the study and randomly allocated into two groups (CRF and PRF). All procedures were performed operation suite with C-arm fluoroscopic guidance. Both, pre- and postprocedure, the patients were assessed for pain on the Visual Analog Scale (VAS) and Barrow Neurological Institute (BNI) Pain Intensity Scale at 1 week and thereafter at 1, 2, 3, and 6 months. Patients with a BNI score ≥4 after 1 month were considered a failure and offered other modes of treatment. A reduction in VAS score ≥50% and a BNI score <4 were considered as effective.
Discreet variables were recorded as proportions, ordinal variables and continuous variables with non-Gaussian distribution as medians with interquartile range, and continuous variables with Gaussian distribution as mean ± standard deviation. Association between ordinal variables was tested by Fisher's exact test/Chi-square test whenever appropriate. Equality of means/median was tested by using paired/unpaired -test or nonparametric tests depending upon the distribution of data. ≤ 0.5 was considered statistically significant. Data analysis was performed using STATA version 13.04 windows.
Efficacy in terms of decrease in VAS ≥50% at 1 month was 33.33% and 83.33% in the PRF and CRF groups, respectively, which was statistically significant( = 0.036). Effective reduction in BNI scores at the 7 day, 1 month, and 2 months postprocedure was evaluated and found in 41.67% and 83.33% of patients in the PRF and CRF groups, respectively, which was statistically insignificant ( = 0.089). There was a statistically significant reduction in BNI scores in PRF and CRF group patients at 3 and 6 months (at 3 months, 33.33% and 83.33%, = 0.036 and at 6 months, 25% and 83.33%, = 0.012). In the CRF group, mild hypoesthesia was evident in three patients which improved by the end of 1 month while no side effects were seen in the PRF group.
CRF is a more effective procedure to decrease pain in comparison to long-duration, fixed voltage PRF for the treatment of idiopathic TGN. Although the side effects are more with CRF, they are mild and self-limiting.

特发性三叉神经痛(TGN)是一种慢性疼痛疾病,会在三叉神经一个或多个分支的分布区域引起单侧、严重的短暂刺痛性复发性疼痛。传统射频(CRF)和脉冲射频(PRF)是两种微创治疗方法。CRF选择性地消融神经节的一部分以缓解疼痛,但已发现它与一些副作用相关,如6%-28%的患者出现感觉异常或感觉丧失,3%-8%的患者出现角膜反射丧失。PRF是一种相对较新的方式,是一种将射频能量传递到半月神经节以产生治疗效果的非破坏性神经调节方法。
我们旨在比较CRF与长时间、固定电压PRF治疗特发性TGN的疗效。
本研究在一家三级医疗中心研究机构进行。
这是一项前瞻性随机试验。
27例成年TGN患者纳入研究并随机分为两组(CRF组和PRF组)。所有操作均在C形臂荧光透视引导下的手术室内进行。术前和术后,在1周时以及此后1、2、3和6个月时,使用视觉模拟量表(VAS)和巴罗神经学研究所(BNI)疼痛强度量表对患者的疼痛进行评估。1个月后BNI评分≥4的患者被视为治疗失败,并提供其他治疗方式。VAS评分降低≥50%且BNI评分<4被视为有效。
离散变量记录为比例,有序变量和非高斯分布的连续变量记录为中位数及四分位数间距,高斯分布的连续变量记录为均值±标准差。适当情况下,有序变量之间的关联通过Fisher精确检验/卡方检验进行。根据数据分布,使用配对/非配对t检验或非参数检验来检验均值/中位数的相等性。P≤0.5被认为具有统计学意义。使用STATA 13.04 Windows版本进行数据分析。
1个月时VAS降低≥50%方面,PRF组和CRF组的疗效分别为33.33%和83.33%,差异具有统计学意义(P = 0.036)。对术后7天、1个月和2个月时BNI评分的有效降低情况进行评估,发现PRF组和CRF组分别有41.67%和83.33%的患者有效,差异无统计学意义(P = 0.089)。PRF组和CRF组患者在3个月和6个月时BNI评分有统计学意义的降低(3个月时,分别为33.33%和83.33%,P = 0.036;6个月时,分别为25%和83.33%,P = 0.012)。CRF组有3例患者出现轻度感觉减退,在1个月末有所改善,而PRF组未观察到副作用。
与长时间、固定电压PRF相比,CRF在治疗特发性TGN时减轻疼痛方面是一种更有效的方法。虽然CRF的副作用更多,但它们是轻微的且具有自限性。