He Lili, Li Hailong, Chen Ming, Wang Jinghua, Altaye Mekibib, Dillman Jonathan R, Parikh Nehal A
Imaging Research Center, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States.
Department of Radiology, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States.
Front Neurosci. 2021 Oct 5;15:753033. doi: 10.3389/fnins.2021.753033. eCollection 2021.
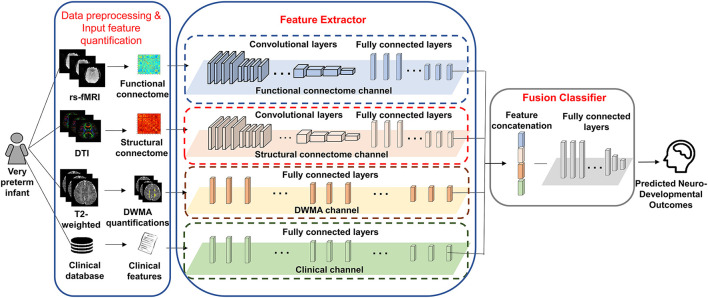
The prevalence of disabled survivors of prematurity has increased dramatically in the past 3 decades. These survivors, especially, very preterm infants (VPIs), born ≤ 32 weeks gestational age, are at high risk for neurodevelopmental impairments. Early and clinically effective personalized prediction of outcomes, which forms the basis for early treatment decisions, is urgently needed during the peak neuroplasticity window-the first couple of years after birth-for at-risk infants, when intervention is likely to be most effective. Advances in MRI enable the noninvasive visualization of infants' brains through acquired multimodal images, which are more informative than unimodal MRI data by providing complementary/supplementary depicting of brain tissue characteristics and pathology. Thus, analyzing quantitative multimodal MRI features affords unique opportunities to study early postnatal brain development and neurodevelopmental outcome prediction in VPIs. In this study, we investigated the predictive power of multimodal MRI data, including T2-weighted anatomical MRI, diffusion tensor imaging, resting-state functional MRI, and clinical data for the prediction of neurodevelopmental deficits. We hypothesize that integrating multimodal MRI and clinical data improves the prediction over using each individual data modality. Employing the aforementioned multimodal data, we proposed novel end-to-end deep multimodal models to predict neurodevelopmental (i.e., cognitive, language, and motor) deficits independently at 2 years corrected age. We found that the proposed models can predict cognitive, language, and motor deficits at 2 years corrected age with an accuracy of 88.4, 87.2, and 86.7%, respectively, significantly better than using individual data modalities. This current study can be considered as proof-of-concept. A larger study with external validation is important to validate our approach to further assess its clinical utility and overall generalizability.
在过去30年中,早产残疾幸存者的患病率急剧上升。这些幸存者,尤其是孕周≤32周出生的极早产儿(VPI),面临神经发育障碍的高风险。在出生后的头几年,即神经可塑性的高峰期,对于有风险的婴儿来说,迫切需要早期且临床有效的个性化结局预测,这是早期治疗决策的基础,此时进行干预可能最有效。MRI的进展使得通过获取的多模态图像对婴儿大脑进行无创可视化成为可能,这些多模态图像通过提供脑组织特征和病理学的互补/补充描绘,比单模态MRI数据更具信息性。因此,分析定量多模态MRI特征为研究VPI出生后脑早期发育和神经发育结局预测提供了独特的机会。在本研究中,我们调查了多模态MRI数据(包括T2加权解剖MRI、扩散张量成像、静息态功能MRI)以及临床数据对神经发育缺陷的预测能力。我们假设整合多模态MRI和临床数据比使用单个数据模态能提高预测效果。利用上述多模态数据,我们提出了新颖的端到端深度多模态模型,以独立预测矫正年龄2岁时的神经发育(即认知、语言和运动)缺陷。我们发现,所提出的模型能够分别以88.4%、87.2%和86.7%的准确率预测矫正年龄2岁时的认知、语言和运动缺陷,显著优于使用单个数据模态。当前这项研究可被视为概念验证。进行一项有外部验证的更大规模研究对于验证我们的方法以进一步评估其临床实用性和总体可推广性很重要。