Health Economics Department, Janssen Pharmaceutical K.K., Tokyo, Japan.
Immunology, Infectious Diseases and Vaccine Department, Medical Affairs Division, Janssen Pharmaceutical K.K., Tokyo, Japan.
Clin Rheumatol. 2022 Mar;41(3):741-755. doi: 10.1007/s10067-021-05939-6. Epub 2021 Oct 22.
INTRODUCTION/OBJECTIVES: Since new consensus on polymyositis (PM) and dermatomyositis (DM) were released in Japan, an updated evidence on treatment landscape and PM/DM burden was essential. This study evaluates treatment burden and overall treatment cost of PM/DM-related inpatient and outpatient visits, treatments, and procedures/patient/year.
This retrospective, observational study analyzed insurance claims from Japan Medical Data Center (JMDC) database. Patients with at least one PM/DM diagnosis/one dispensation of treatment between 1 January 2009 and 31 December 2019 were enrolled. Patient characteristics, treatment patterns and sequence, treatment choices, healthcare resource utilization (HCRU), and related costs were assessed. Chi-square test and linear regression model were used to assess impact of patient characteristics on treatment choice.
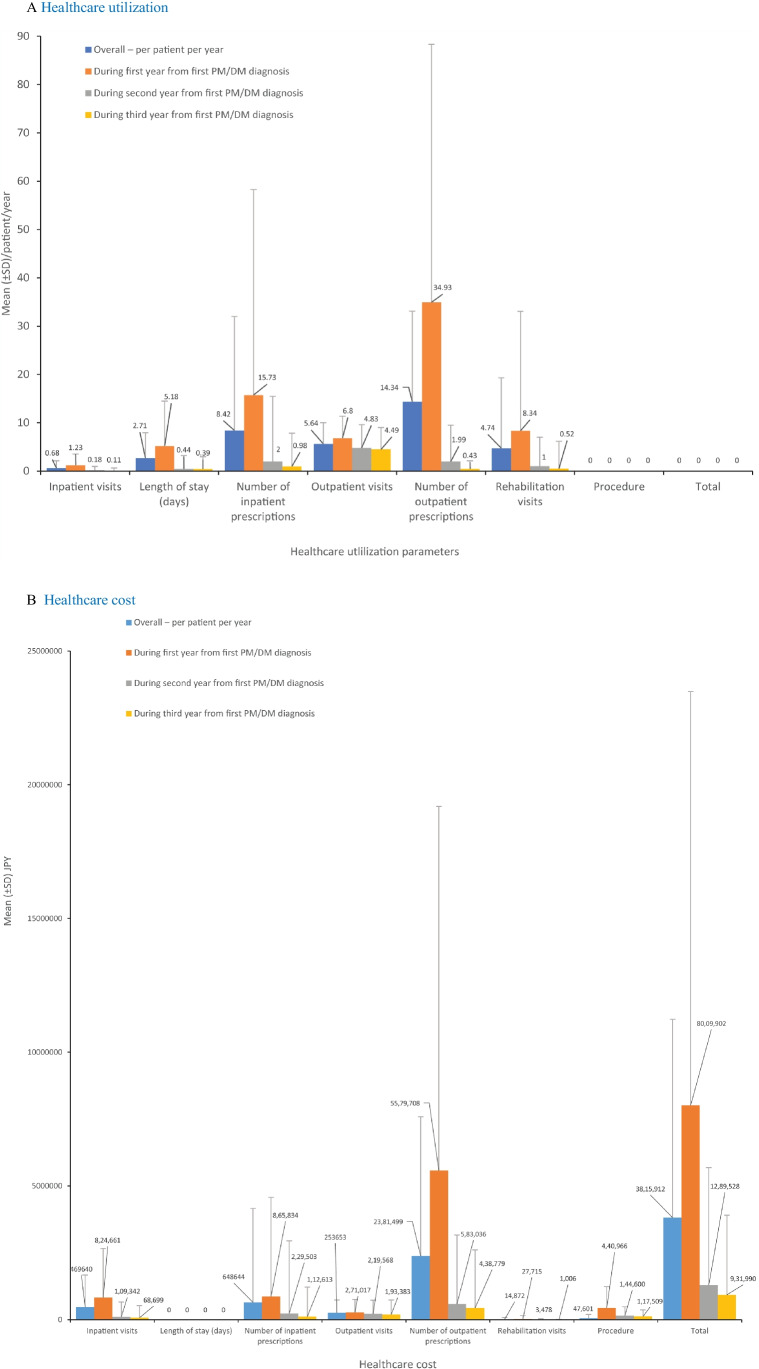
Patients (836/4,961) receiving a relevant treatment were analyzed. Heart disease (35%), interstitial lung disease (27%), and diabetes mellitus (26%) were frequently identified as comorbidities. Concomitant dispensation of immunosuppressants and systemic steroids was largely found in first and second line of treatment (LoT) while systemic steroids remained as single dominant treatment across all LoTs. HCRU was very low for inpatient visits (0.68 [1.43]) or rehabilitation (4.74 [14.57]). The mean (SD) number of inpatient visits decreased from first (1.23 [2.32]) to third year (0.11 [0.54]). Total mean (SD) healthcare cost per patients per year was ¥ 3,815,912 (7,412,241), with overall drug dispensation compounding to 80% of total cost.
High concomitant immunosuppressant and systemic steroid prescriptions in first LoT recommend early optimal treatment to manage PM/DM. Although inpatient costs are low, outpatient dispensation costs increase overall economic burden.
简介/目的:自日本发布关于多发性肌炎(PM)和皮肌炎(DM)的新共识以来,有必要提供关于治疗现状和 PM/DM 负担的最新证据。本研究评估了 PM/DM 相关住院和门诊就诊、治疗和程序/患者/年的治疗负担和总体治疗费用。
这是一项回顾性、观察性研究,分析了日本医疗数据中心(JMDC)数据库中的保险索赔。纳入了 2009 年 1 月 1 日至 2019 年 12 月 31 日期间至少有一次 PM/DM 诊断/一次治疗配药的患者。评估了患者特征、治疗模式和顺序、治疗选择、医疗资源利用(HCRU)和相关费用。使用卡方检验和线性回归模型评估患者特征对治疗选择的影响。
分析了接受相关治疗的患者(836/4961)。经常发现合并症包括心脏病(35%)、间质性肺病(27%)和糖尿病(26%)。免疫抑制剂和全身皮质类固醇的同时配药在一线和二线治疗(LoT)中大量发现,而全身皮质类固醇在所有 LoT 中仍然是单一主导治疗。住院就诊(0.68[1.43])或康复就诊(4.74[14.57])的 HCRU 非常低。第 1 年(1.23[2.32])和第 3 年(0.11[0.54])的住院就诊平均(SD)次数减少。每位患者每年的平均(SD)医疗保健费用为 3815912 日元(7412241 日元),总药物配药费用占总费用的 80%。
一线治疗中高比例的免疫抑制剂和全身皮质类固醇处方建议早期进行最佳治疗以管理 PM/DM。尽管住院费用较低,但门诊配药费用增加了整体经济负担。