Department of Medicine, Wake Forest School of Medicine, Winston-Salem, NC 27101, USA.
The Department of Medicine, Rowan School of Osteopathic Medicine, Stratford, NJ 08084, USA.
Int J Mol Sci. 2021 Oct 19;22(20):11270. doi: 10.3390/ijms222011270.
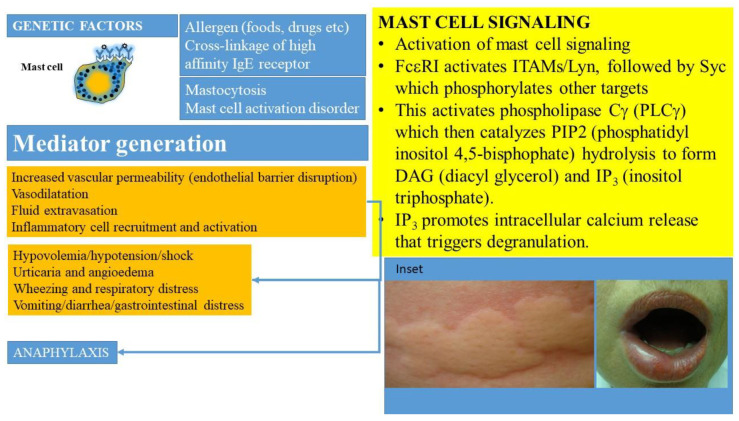
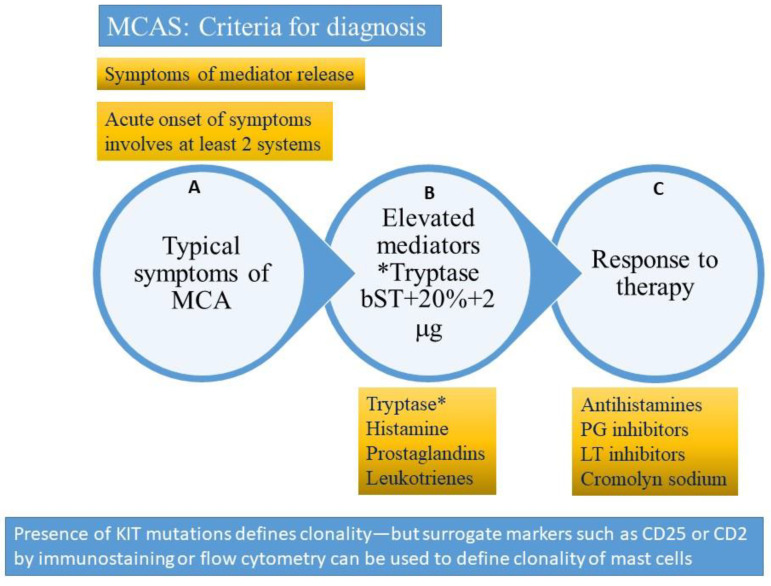
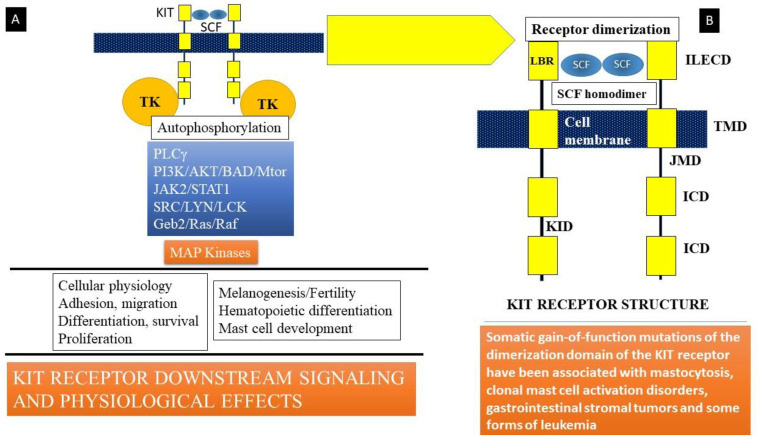
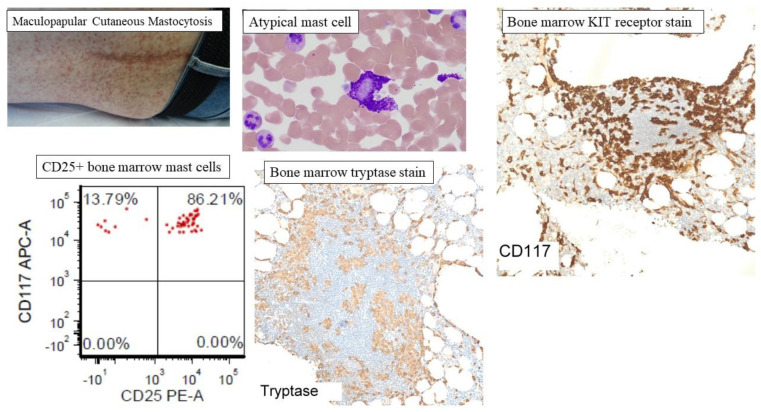
Mast cells are derived from hematopoietic stem cell precursors and are essential to the genesis and manifestations of the allergic response. Activation of these cells by allergens leads to degranulation and elaboration of inflammatory mediators, responsible for regulating the acute dramatic inflammatory response seen. Mast cells have also been incriminated in such diverse disorders as malignancy, arthritis, coronary artery disease, and osteoporosis. There has been a recent explosion in our understanding of the mast cell and the associated clinical conditions that affect this cell type. Some mast cell disorders are associated with specific genetic mutations (such as the D816V gain-of-function mutation) with resultant clonal disease. Such disorders include cutaneous mastocytosis, systemic mastocytosis (SM), its variants (indolent/ISM, smoldering/SSM, aggressive systemic mastocytosis/ASM) and clonal (or monoclonal) mast cell activation disorders or syndromes (CMCAS/MMAS). Besides clonal mast cell activations disorders/CMCAS (also referred to as monoclonal mast cell activation syndromes/MMAS), mast cell activation can also occur secondary to allergic, inflammatory, or paraneoplastic disease. Some disorders are idiopathic as their molecular pathogenesis and evolution are unclear. A genetic disorder, referred to as hereditary alpha-tryptasemia (HαT) has also been described recently. This condition has been shown to be associated with increased severity of allergic and anaphylactic reactions and may interact variably with primary and secondary mast cell disease, resulting in complex combined disorders. The role of this review is to clarify the classification of mast cell disorders, point to molecular aspects of mast cell signaling, elucidate underlying genetic defects, and provide approaches to targeted therapies that may benefit such patients.
肥大细胞来源于造血干细胞前体,是过敏反应的发生和表现所必需的。过敏原激活这些细胞会导致脱颗粒和炎症介质的产生,这些介质负责调节所观察到的急性剧烈炎症反应。肥大细胞也与恶性肿瘤、关节炎、冠状动脉疾病和骨质疏松症等多种疾病有关。近年来,我们对肥大细胞及其相关临床病症的理解有了突飞猛进的发展,这些病症影响着这种细胞类型。一些肥大细胞疾病与特定的遗传突变(如 D816V 获得性功能突变)有关,导致克隆性疾病。这些疾病包括皮肤肥大细胞增多症、系统性肥大细胞增多症(SM)、其变体(惰性/ISM、潜伏/SSM、侵袭性系统性肥大细胞增多症/ASM)以及克隆(或单克隆)肥大细胞激活障碍或综合征(CMCAS/MMAS)。除了克隆性肥大细胞激活障碍/CMCAS(也称为单克隆肥大细胞激活综合征/MMAS)外,肥大细胞激活也可能继发于过敏、炎症或副肿瘤性疾病。一些疾病是特发性的,因为它们的分子发病机制和演变尚不清楚。最近还描述了一种遗传性疾病,称为遗传性α-胰蛋白酶血症(HαT)。这种情况已被证明与过敏和过敏反应的严重程度增加有关,并且可能与原发性和继发性肥大细胞疾病相互作用,导致复杂的联合疾病。本综述的目的是阐明肥大细胞疾病的分类,指出肥大细胞信号转导的分子方面,阐明潜在的遗传缺陷,并提供针对这些患者可能有益的靶向治疗方法。