Department of Pathophysiology, University of Medicine, Pharmacology, Sciences and Technology, 540142 Târgu-Mureș, Romania.
Department of Anesthesiology and Intensive Care, Emergency County Hospital, 540136 Târgu-Mureș, Romania.
Medicina (Kaunas). 2021 Oct 19;57(10):1132. doi: 10.3390/medicina57101132.
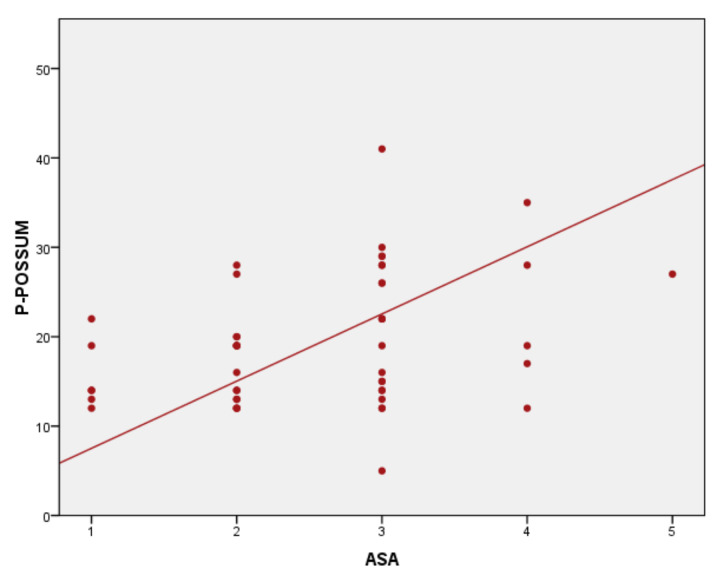
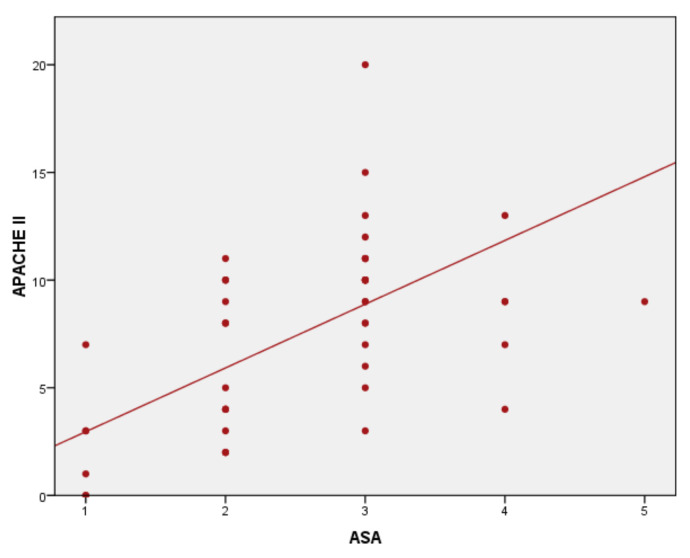
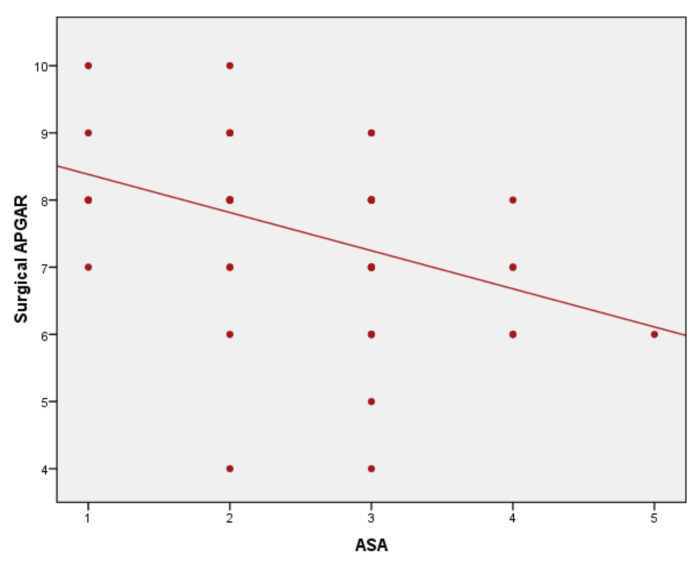
: Numerous scoring systems have been introduced into modern medicine. None of the scoring systems assessed both anesthetic and surgical risk of the patient, predict the morbidity, mortality, or the need for postoperative intensive care unit admission. The aim of this study was to compare the anesthetic and surgical scores currently used, for a better evaluation of perioperative risks, morbidity, and mortality. : This is a pilot, prospective, observational study. We enrolled 50 patients scheduled for elective surgery. Anesthetic and surgery risk was assessed using American Society of Anesthesiologists (ASA) scale, Physiological and Operative Severity Score for the enumeration of Mortality and morbidity (P-POSSUM), Acute Physiology and Chronic Health Evaluation (APACHE II), and Surgical APGAR Score (SAS) scores. The real and the estimated length of stay (LOS) were registered. : We obtained several statistically significant positive correlations: ASA score-P-POSSUM ( < 0.01, r = 0.465); ASA score-SAS, ( < 0.01, r = -0.446); ASA score-APACHE II, ( < 0.01 r = 0.519); predicted LOS and ASA score ( < 0.01, r = 0.676); predicted LOS and -POSSUM ( < 0.01, r = 0.433); and predicted LOS and APACHE II ( < 0.01, r = 0.454). A significant negative correlation between predicted LOS, real LOS, ASA class, and SAS ( < 0.05) was observed. We found a statistically significant difference between the predicted and actual LOS ( < 001). : Anesthetic, surgical, and severity scores, used together, provide clearer information about mortality, morbidity, and LOS. ASA scale, associated with surgical scores and severity scores, presents a better image of the patient's progress in the perioperative period. In our study, APACHE II is the best predictor of mortality, followed by P-POSSUM and SAS. P-POSSUM score and ASA scale may be complementary in terms of preoperative physiological factors, providing valuable information for postoperative outcomes.
许多评分系统已经被引入现代医学。目前还没有任何评分系统能够同时评估患者的麻醉和手术风险,预测发病率、死亡率或术后入住重症监护病房的需求。本研究旨在比较目前使用的麻醉和手术评分,以便更好地评估围手术期风险、发病率和死亡率。
这是一项前瞻性、观察性的研究。我们招募了 50 名计划接受择期手术的患者。使用美国麻醉师协会(ASA)评分、生理和手术严重程度评分预测死亡率和发病率(P-POSSUM)、急性生理学和慢性健康评估(APACHE II)以及手术 APGAR 评分(SAS)评估麻醉和手术风险。记录实际和估计的住院时间(LOS)。
ASA 评分-P-POSSUM(<0.01,r=0.465);ASA 评分-SAS(<0.01,r=-0.446);ASA 评分-APACHE II(<0.01,r=0.519);预测 LOS 和 ASA 评分(<0.01,r=0.676);预测 LOS 和-POSSUM(<0.01,r=0.433);以及预测 LOS 和 APACHE II(<0.01,r=0.454)。观察到预测 LOS、实际 LOS、ASA 分级和 SAS 之间存在显著负相关(<0.05)。我们发现预测和实际 LOS 之间存在统计学显著差异(<0.01)。
麻醉、手术和严重程度评分一起使用,提供了关于死亡率、发病率和 LOS 的更清晰信息。ASA 分级与手术评分和严重程度评分相结合,更好地反映了患者围手术期的进展情况。在我们的研究中,APACHE II 是死亡率的最佳预测指标,其次是 P-POSSUM 和 SAS。P-POSSUM 评分和 ASA 分级在术前生理因素方面可能具有互补性,为术后结局提供有价值的信息。