Cuijpers Anne C M, Coolsen Marielle M E, Schnabel Ronny M, van Santen Susanne, Olde Damink Steven W M, van de Poll Marcel C G
Department of Surgery, Maastricht University Medical Centre+, Postbus 5800, 6202 AZ, Maastricht, The Netherlands.
Intensive Care Department, Maastricht University Medical Centre+, Postbus 5800, 6202 AZ, Maastricht, The Netherlands.
World J Surg. 2020 Dec;44(12):4060-4069. doi: 10.1007/s00268-020-05742-5. Epub 2020 Aug 30.
Postoperative outcome prediction in elderly is based on preoperative physical status but its predictive value is uncertain. The goal was to evaluate the value of risk assessment performed perioperatively in predicting outcome in case of admission to an intensive care unit (ICU).
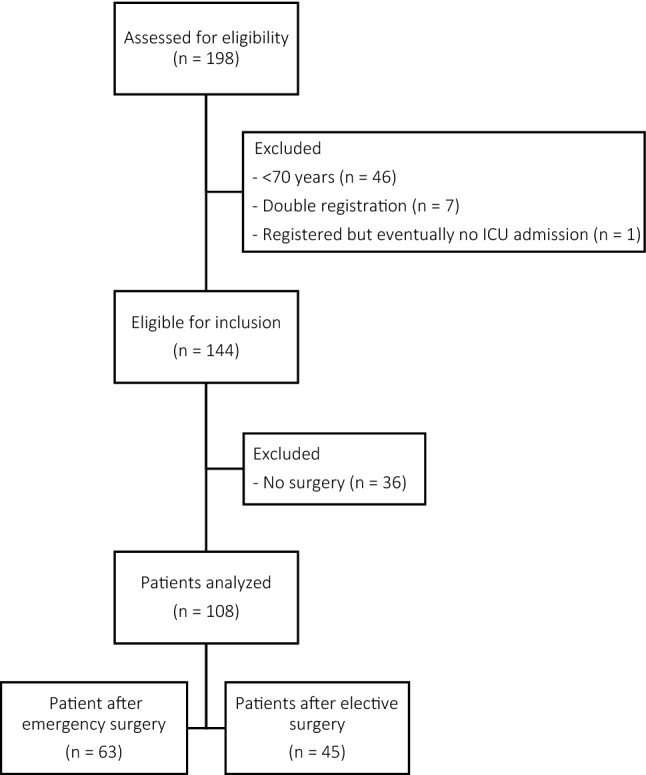
A total of 108 postsurgical patients were retrospectively selected from a prospectively recorded database of 144 elderly septic patients (>70 years) admitted to the ICU department after elective or emergency abdominal surgery between 2012 and 2017. Perioperative risk assessment scores including Portsmouth Physiological and Operative Severity Score for the enumeration of Mortality (P-POSSUM) and American Society of Anaesthesiologists Physical Status classification (ASA) were determined. Acute Physiology and Chronic Health Evaluation IV (APACHE IV) was obtained at ICU admission.
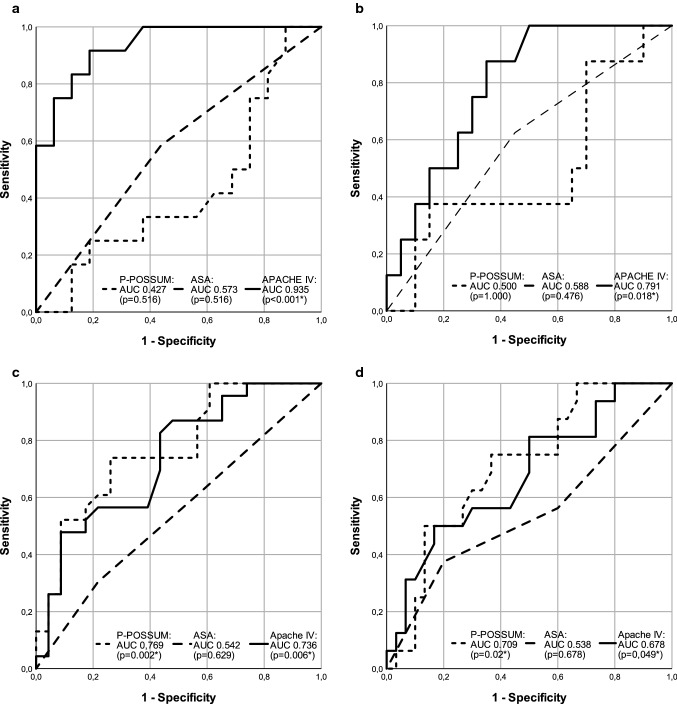
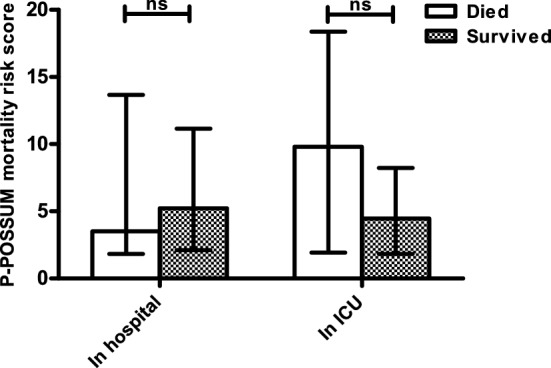
In-hospital mortality was 48.9% in elderly requiring ICU admission after elective surgery (n = 45), compared to 49.2% after emergency surgery (n = 63). APACHE IV significantly predicted in-hospital mortality after complicated elective surgery [area under the curve 0.935 (p < 0.001)] where outpatient ASA physical status and P-POSSUM did not. In contrast, P-POSSUM and APACHE IV significantly predicted in-hospital mortality when based on current physical state in elderly requiring emergency surgery (AUC 0.769 (p = 0.002) and 0.736 (p = 0.006), respectively).
Perioperative risk assessment reflecting premorbid physical status of elderly loses its value when complications occur requiring unplanned ICU admission. Risks in elderly should be re-assessed based on current clinical condition prior to ICU admission, because outcome prediction is more reliable then.
老年人术后结局预测基于术前身体状况,但其预测价值尚不确定。目的是评估围手术期进行的风险评估对预测入住重症监护病房(ICU)患者结局的价值。
从2012年至2017年间因择期或急诊腹部手术后入住ICU的144例老年脓毒症患者(>70岁)的前瞻性记录数据库中,回顾性选取了108例术后患者。确定围手术期风险评估评分,包括用于计算死亡率的朴茨茅斯生理和手术严重程度评分(P-POSSUM)以及美国麻醉医师协会身体状况分类(ASA)。在ICU入院时获取急性生理与慢性健康状况评估IV(APACHE IV)。
择期手术后需要入住ICU的老年人院内死亡率为48.9%(n = 45),急诊手术后为49.2%(n = 63)。APACHE IV显著预测了复杂择期手术后的院内死亡率[曲线下面积0.935(p < 0.001)],而门诊ASA身体状况和P-POSSUM则不能。相比之下,当基于需要急诊手术的老年人当前身体状态时,P-POSSUM和APACHE IV显著预测了院内死亡率(曲线下面积分别为0.769(p = 0.002)和0.736(p = 0.006))。
反映老年人病前身体状况的围手术期风险评估在出现需要意外入住ICU的并发症时失去其价值。老年人的风险应在入住ICU前根据当前临床状况重新评估,因为此时结局预测更可靠。