Kisa Nagihan Gozde, Kisa Emre, Cevik Banu Eler
Anesthesiology and Reanimation, Golcuk Necati Celik State Hospital, Kocaeli, TUR.
Anesthesiology and Critical Care, Derince Education and Research Hospital, Kocaeli, TUR.
Cureus. 2021 Mar 4;13(3):e13684. doi: 10.7759/cureus.13684.
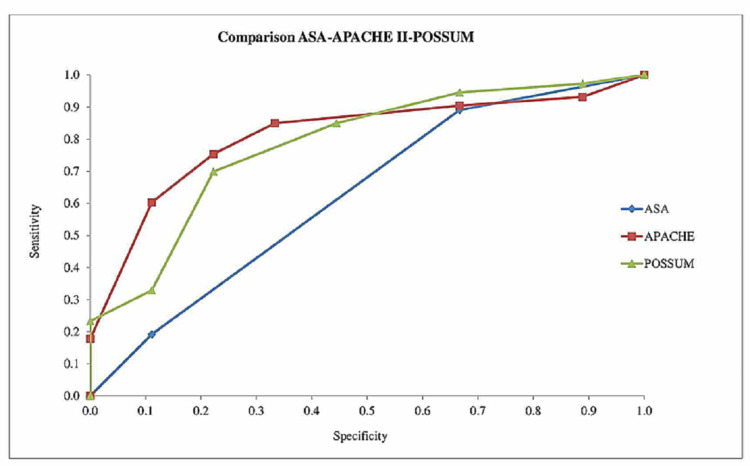
Scoring systems have been developed to predict the expected mortality and morbidity in surgical procedures. In this study, our aim was to compare the ASA (American Society of Anesthesiologists), APACHE (Acute Physiology and Chronic Health Evaluation) II, POSSUM (Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity) scoring systems as predictors of mortality in patients who underwent gastrointestinal oncologic surgery, followed, and were admitted to the intensive care unit during the postoperative period. We examined the files of 82 patients who underwent oncologic gastrointestinal surgery and followed up in the intensive care units (ICUs). The patients' APACHE II scores and predicted mortality rates (PMR) according to the APACHE II, POSSUM, and ASA scores were calculated. The receiver operator characteristic (ROC) curve analysis was used when evaluating the performances of the ASA, APACHE, and POSSUM scoring systems in terms of accurate assessment of mortality. Accordingly, the area under the curve (AUC) = 0.5 no distinction, 0.5 <AUC <0.7 discriminative power of the test is statistically not significant, 0.7 <AUC <0.8 acceptable, 0.8 <AUC <0.9 very good and 0.9 <AUC <1 perfect. The evaluations showed that APACHE II had the best performance with 0.81, followed by POSSUM, which had an acceptable level at 0.78. On the other hand, the ASA score was 0.63 and its discriminative power was identified as statistically insignificant. Our results show that the POSSUM and APACHE II scoring systems were better at predicting mortality than the ASA scoring system for the prediction of mortality in the postoperative period. Both the POSSUM and APACHE II scoring systems can be confidently used for the prediction of mortality in patients undergoing operations due to oncologic gastrointestinal diseases.
已经开发出评分系统来预测外科手术中预期的死亡率和发病率。在本研究中,我们的目的是比较美国麻醉医师协会(ASA)、急性生理与慢性健康状况评估系统(APACHE)II、手术死亡率和发病率评估系统(POSSUM)这三种评分系统,以预测接受胃肠肿瘤手术、术后接受随访并入住重症监护病房的患者的死亡率。我们检查了82例接受肿瘤胃肠手术并在重症监护病房(ICU)接受随访的患者的病历。根据APACHE II、POSSUM和ASA评分计算患者的APACHE II评分和预测死亡率(PMR)。在评估ASA、APACHE和POSSUM评分系统对死亡率的准确评估性能时,使用了受试者工作特征(ROC)曲线分析。因此,曲线下面积(AUC)=0.5无区分能力,0.5<AUC<0.7测试的区分能力在统计学上不显著,0.7<AUC<0.8可接受,0.8<AUC<0.9非常好,0.9<AUC<1完美。评估显示,APACHE II的表现最佳,AUC为0.81,其次是POSSUM,其AUC为0.78,处于可接受水平。另一方面,ASA评分为0.63,其区分能力在统计学上不显著。我们的结果表明,在预测术后死亡率方面,POSSUM和APACHE II评分系统比ASA评分系统更能准确预测死亡率。POSSUM和APACHE II评分系统都可以可靠地用于预测因胃肠肿瘤疾病接受手术患者的死亡率。