International Diabetes Center, HealthPartners Institute, Minneapolis, Minnesota, USA.
Yale University School of Medicine Pediatric Endocrinology, New Haven, Connecticut, USA.
Diabetes Technol Ther. 2022 Mar;24(3):178-189. doi: 10.1089/dia.2021.0319. Epub 2021 Nov 16.
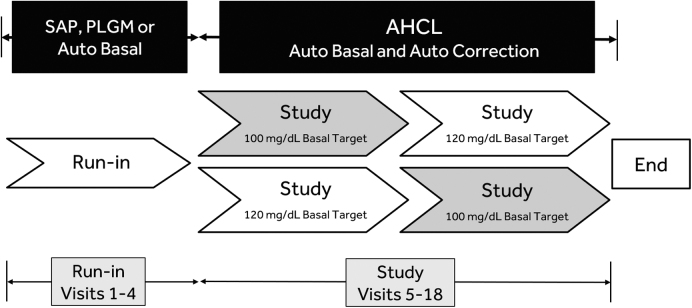
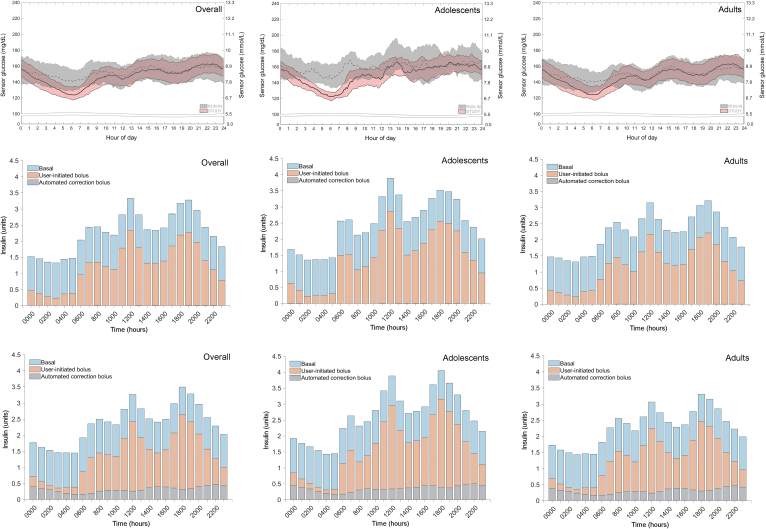
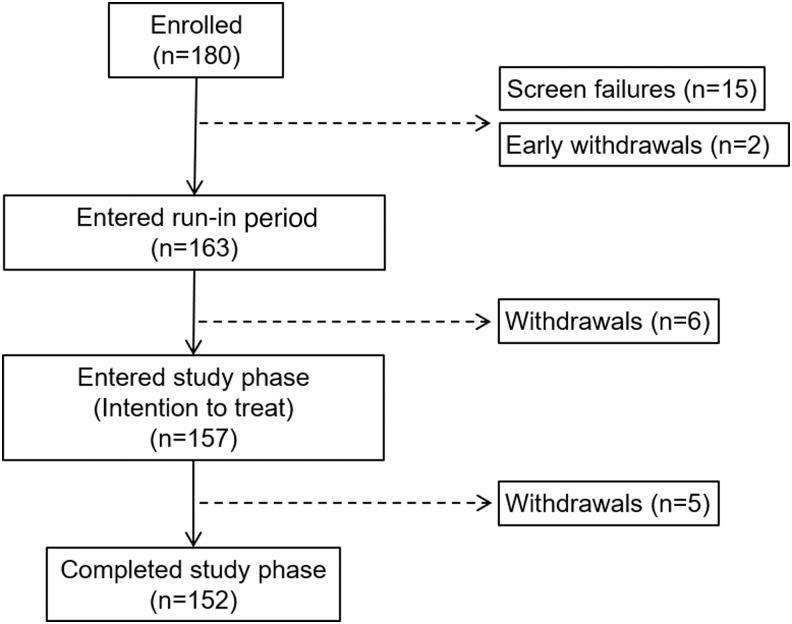
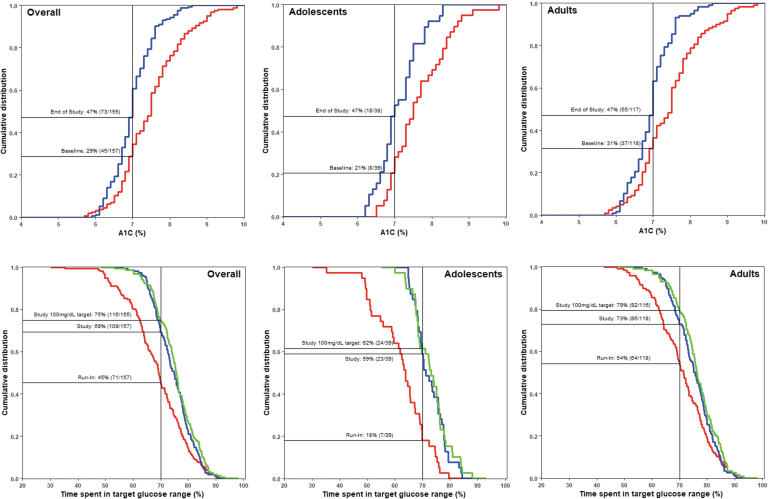
This trial assessed safety and effectiveness of an advanced hybrid closed-loop (AHCL) system with automated basal (Auto Basal) and automated bolus correction (Auto Correction) in adolescents and adults with type 1 diabetes (T1D). This multicenter single-arm study involved an intent-to-treat population of 157 individuals (39 adolescents aged 14-21 years and 118 adults aged ≥22-75 years) with T1D. Study participants used the MiniMed™ AHCL system during a baseline run-in period in which sensor-augmented pump +/- predictive low glucose management or Auto Basal was enabled for ∼14 days. Thereafter, Auto Basal and Auto Correction were enabled for a study phase (∼90 days), with glucose target set to 100 or 120 mg/dL for ∼45 days, followed by the other target for ∼45 days. Study endpoints included safety events and change in mean A1C, time in range (TIR, 70-180 mg/dL) and time below range (TBR, <70 mg/dL). Run-in and study phase values were compared using Wilcoxon signed-rank test or paired -test. Overall group time spent in closed loop averaged 94.9% ± 5.4% and involved only 1.2 ± 0.8 exits per week. Compared with run-in, AHCL reduced A1C from 7.5% ± 0.8% to 7.0% ± 0.5% (<0.001, Wilcoxon signed-rank test, = 155), TIR increased from 68.8% ± 10.5% to 74.5% ± 6.9% (<0.001, Wilcoxon signed-rank test), and TBR reduced from 3.3% ± 2.9% to 2.3% ± 1.7% (<0.001, Wilcoxon signed-rank test). Similar benefits to glycemia were observed for each age group and were more pronounced for the nighttime (12 AM-6 AM). The 100 mg/dL target increased TIR to 75.4% ( = 155), which was further optimized at a lower active insulin time (AIT) setting (i.e., 2 h), without increasing TBR. There were no severe hypoglycemic or diabetic ketoacidosis events during the study phase. These findings show that the MiniMed AHCL system is safe and allows for achievement of recommended glycemic targets in adolescents and adults with T1D. Adjustments in target and AIT settings may further optimize glycemia and improve user experience. Clinical Trial Registration number: NCT03959423.
这项试验评估了一种具有自动基础(Auto Basal)和自动推注校正(Auto Correction)功能的先进混合闭环(AHCL)系统在 1 型糖尿病(T1D)青少年和成人患者中的安全性和有效性。这是一项多中心、单臂研究,共纳入 157 名 T1D 患者(39 名 14-21 岁的青少年和 118 名≥22-75 岁的成年人)作为意向治疗人群。在基线入组期间,研究参与者使用 MiniMed™AHCL 系统,在此期间,传感器增强型泵 +/-预测性低血糖管理或 Auto Basal 可使用约 14 天。此后,启用 Auto Basal 和 Auto Correction 进行研究阶段(约 90 天),血糖目标设定为 100 或 120mg/dL 约 45 天,然后设定另一个目标约 45 天。研究终点包括安全性事件和平均 A1C 的变化、血糖达标时间(TIR,70-180mg/dL)和血糖不达标的时间(TBR,<70mg/dL)。使用 Wilcoxon 符号秩检验或配对 t 检验比较入组和研究阶段的值。总体上,闭环时间的平均值为 94.9%±5.4%,每周仅需要 1.2±0.8 次退出。与入组相比,AHCL 将 A1C 从 7.5%±0.8%降低至 7.0%±0.5%(<0.001,Wilcoxon 符号秩检验,n=155),TIR 从 68.8%±10.5%增加至 74.5%±6.9%(<0.001,Wilcoxon 符号秩检验),TBR 从 3.3%±2.9%降低至 2.3%±1.7%(<0.001,Wilcoxon 符号秩检验)。每个年龄组的血糖都有类似的改善,夜间(12 AM-6 AM)的改善更为明显。100mg/dL 的目标将 TIR 提高至 75.4%(n=155),通过将活性胰岛素时间(AIT)设置更改为 2 小时(即 2 小时)进一步优化,而不会增加 TBR。研究期间没有发生严重低血糖或糖尿病酮症酸中毒事件。这些发现表明,MiniMed AHCL 系统是安全的,并允许 T1D 青少年和成人达到推荐的血糖目标。目标和 AIT 设置的调整可能进一步优化血糖,并改善用户体验。临床试验注册号:NCT03959423。