Laboratory of Adjuvant and Antigen Research, US Military HIV Research Program, Walter Reed Army Institute of Research, Silver Spring, MD 20910, USA.
Institute of Human Virology, University of Maryland School of Medicine, Baltimore, MD 21201, USA.
Viruses. 2021 Oct 14;13(10):2074. doi: 10.3390/v13102074.
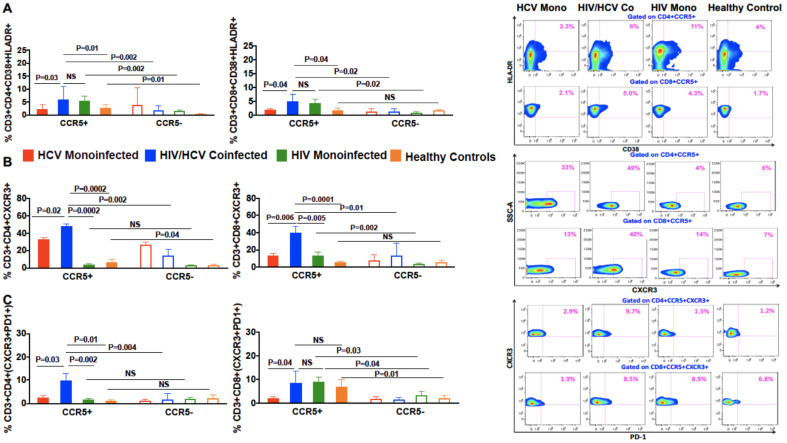
Liver fibrosis is accelerated in patients coinfected with hepatitis C virus and human immunodeficiency virus (HIV), compared with HCV monoinfected patients, although the underlying mechanisms are unknown. We hypothesize that T cells expressing the HIV co-receptor, chemokine receptor 5 (CCR5), preferentially migrate to the inflamed liver and contribute to enhanced fibrogenesis. We compared the peripheral and intrahepatic CCR5 expression on CD4+ and CD8+ T cells in 21 HIV/HCV-coinfected patients with 14 chronic HCV monoinfected patients. Using 12-color flow cytometry, phenotypic and functional characterization of CCR5+ and negative cells pre- and post-stimulation with HCV genotype specific overlapping pooled peptides was conducted. Patients with HIV/HCV coinfection had significantly more CD4+CCR5+ and CD8+CCR5+ T cells in the liver as compared with peripheral blood ( = 0.0001 for both). Compared with patients with HCV monoinfection, patients with HIV/HCV coinfection also had fewer peripheral CD4+CCR5+ and CD8+CCR5+ T cells ( = 0.02, = 0.001 respectively), but more intrahepatic CD4+CCR5+ and CD8+CCR5+ cells ( = 0.0001 for both). Phenotypic analysis of CCR5+ sorted cells demonstrated an increased expression of markers of exhaustion, senescence, immune activation and liver homing (PD1, CD57, CD38, HLADR, and CXCR3). Post-stimulation with HCV peptides, CCR5+ T cells secreted more proinflammatory and profibrogenic cytokines and chemokines rather than antiviral cytokines. Phenotypic and functional analyses of CCR5+ T cells in HIV/HCV-coinfected patients revealed a pathogenic role for CCR5+ T cells in hepatic fibrogenesis. These cells are functionally proinflammatory, pro-fibrogenic and preferentially accumulate in liver, accelerating fibrosis. These findings suggest that targeting CCR5 may be a therapeutic strategy for be ameliorating liver fibrosis.
丙型肝炎病毒(HCV)和人类免疫缺陷病毒(HIV)合并感染患者的肝纤维化进展较 HCV 单感染患者更快,但其潜在机制尚不清楚。我们假设表达 HIV 辅助受体趋化因子受体 5(CCR5)的 T 细胞优先迁移至炎症肝组织,并促进肝纤维化的发生。我们比较了 21 例 HIV/HCV 合并感染患者和 14 例慢性 HCV 单感染患者外周血和肝组织中 CD4+和 CD8+T 细胞的 CCR5 表达。采用 12 色流式细胞术,对 HCV 基因型特异性重叠多肽预刺激和刺激后 CCR5+和阴性细胞的表型和功能进行了特征分析。与外周血相比,HIV/HCV 合并感染患者肝组织中 CD4+CCR5+和 CD8+CCR5+T 细胞明显更多(均 0.0001)。与 HCV 单感染患者相比,HIV/HCV 合并感染患者外周血中 CD4+CCR5+和 CD8+CCR5+T 细胞也更少(均 0.02, 0.001),但肝内 CD4+CCR5+和 CD8+CCR5+T 细胞更多(均 0.0001)。CCR5+分选细胞的表型分析显示,衰竭、衰老、免疫激活和肝归巢标志物(PD1、CD57、CD38、HLA-DR 和 CXCR3)的表达增加。用 HCV 肽刺激后,CCR5+T 细胞分泌更多促炎和促纤维化细胞因子和趋化因子,而不是抗病毒细胞因子。HIV/HCV 合并感染患者 CCR5+T 细胞的表型和功能分析显示,CCR5+T 细胞在肝纤维化发病机制中发挥致病作用。这些细胞具有促炎、促纤维化功能,并且优先聚集在肝脏中,加速纤维化。这些发现提示,靶向 CCR5 可能是改善肝纤维化的一种治疗策略。