Odenwald Birgit, Fischer Aline, Röschinger Wulf, Liebl Bernhard, Schmidt Heinrich, Nennstiel Uta
Newborn Screening Centre/State Institute of Health, Bavarian Health and Food Safety Authority, 85764 Oberschleissheim, Germany.
Paediatric and Youth Medicine Clinic, Klinikum Dritter Orden, 80638 Munich, Germany.
Int J Neonatal Screen. 2021 Oct 13;7(4):65. doi: 10.3390/ijns7040065.
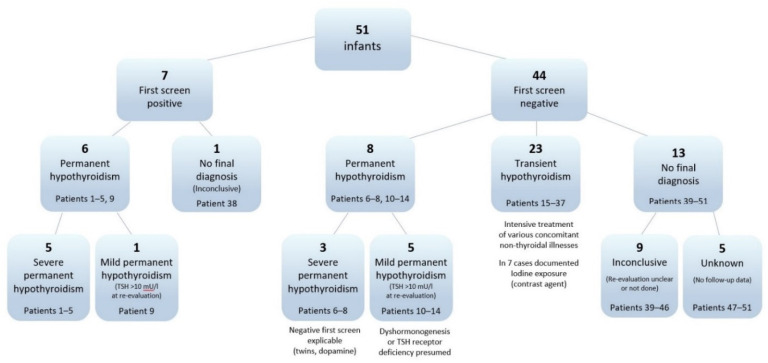
After several decades of successful newborn screening (NBS) for congenital hypothyroidism, the optimal hypothyroidism NBS algorithm for very preterm infants is still controversial. Due to concerns about an elevated risk of a false-negative initial thyroid-stimulation hormone (TSH) screening, repeat NBS has been implemented for this group. While transient hypothyroidism is known to be more frequent among very preterm infants, the prevalence of permanent hypothyroidism is generally assumed to be the same as in more mature newborns. This study analyses screening and long-term follow-up data from the population-based cohort of 51 infants born from 1999-2017 at less than 32 weeks of gestation and diagnosed with hypothyroidism after NBS in the German Federal State of Bavaria (total number of infants screened 2,107,864). Severe permanent hypothyroidism was always detected at initial TSH screening unless there was a known confounding factor. Cases detected by repeat screening after a negative initial screen most frequently proved to be transient, less frequently mild permanent, or a definitive diagnosis was not possible because of inadequate re-evaluation of the thyroid axis. The prevalence of both permanent and transient hypothyroidism was elevated compared to a cohort of children from the same region born at a higher gestational age. The results seem to support the need for the repeated NBS of very preterm infants. However, as the recommendation to treat mild hypothyroidism is not based on high quality evidence, important issues for future research include treatment outcome studies or even a general review of whether this diagnosis meets the screening criteria. Meanwhile, involving a paediatric endocrinologist in treatment decisions is crucial for optimising the benefit of hypothyroidism screening for this particularly vulnerable group.
在先天性甲状腺功能减退症的新生儿筛查(NBS)成功开展数十年后,针对极早产儿的最佳甲状腺功能减退症NBS算法仍存在争议。由于担心初次甲状腺刺激激素(TSH)筛查出现假阴性的风险升高,已对该群体实施了重复NBS。虽然已知短暂性甲状腺功能减退症在极早产儿中更为常见,但一般认为永久性甲状腺功能减退症的患病率与足月新生儿相同。本研究分析了1999年至2017年在德国巴伐利亚州出生、孕周小于32周且在NBS后被诊断为甲状腺功能减退症的51名婴儿的基于人群队列的筛查和长期随访数据(筛查婴儿总数为2,107,864)。除非存在已知的混杂因素,严重永久性甲状腺功能减退症总是在初次TSH筛查时被检测到。初次筛查阴性后通过重复筛查检测出的病例,大多数被证明是短暂性的,较少是轻度永久性的,或者由于甲状腺轴重新评估不充分而无法做出明确诊断。与同一地区孕周较大出生的儿童队列相比,永久性和短暂性甲状腺功能减退症的患病率均有所升高。结果似乎支持对极早产儿进行重复NBS的必要性。然而,由于治疗轻度甲状腺功能减退症的建议并非基于高质量证据,未来研究的重要问题包括治疗结果研究,甚至对该诊断是否符合筛查标准进行全面审查。同时,让儿科内分泌学家参与治疗决策对于优化这一特别脆弱群体的甲状腺功能减退症筛查益处至关重要。