Institute of Metabolism and Systems Research, University of Birmingham, Birmingham, UK.
Department of Endocrinology, Queen Elizabeth Hospital, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
Eur J Endocrinol. 2021 Nov 30;186(1):25-36. doi: 10.1530/EJE-21-0510.
Adrenocortical carcinoma (ACC) has an aggressive but variable clinical course. Prognostic stratification based on the European Network for the Study of Adrenal Tumours stage and Ki67 index is limited. We aimed to demonstrate the prognostic role of a points-based score (S-GRAS) in a large cohort of patients with ACC.
This is a multicentre, retrospective study on ACC patients who underwent adrenalectomy.
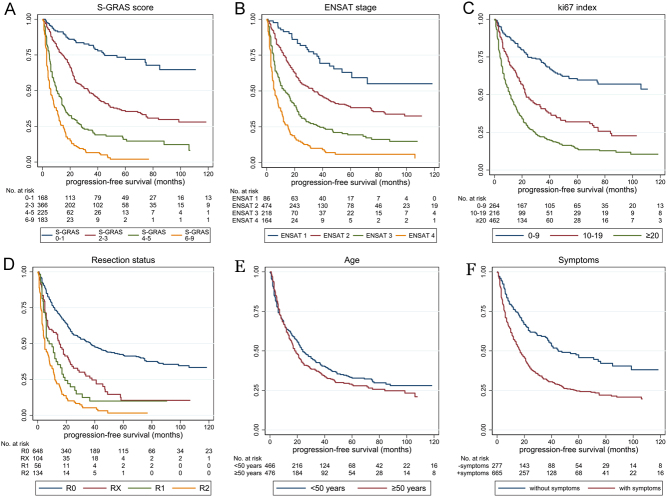
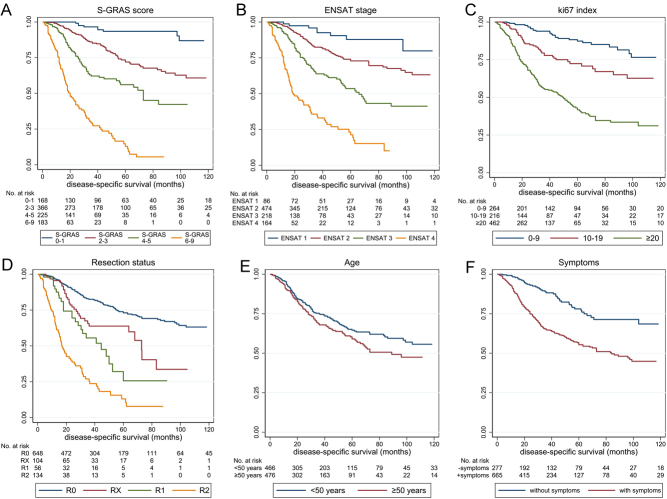
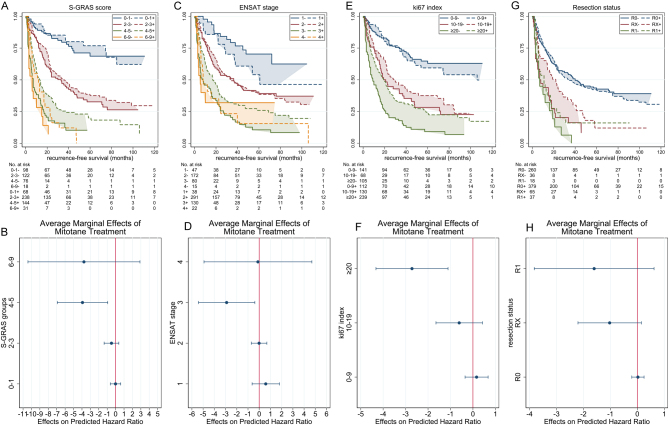
The S-GRAS score was calculated as a sum of the following points: tumour stage (1-2 = 0; 3 = 1; 4 = 2), grade (Ki67 index 0-9% = 0; 10-19% = 1; ≥20% = 2 points), resection status (R0 = 0; RX = 1; R1 = 2; R2 = 3), age (<50 years = 0; ≥50 years = 1), symptoms (no = 0; yes = 1), and categorised, generating four groups (0-1, 2-3, 4-5, and 6-9). Endpoints were progression-free survival (PFS) and disease-specific survival (DSS). The discriminative performance of S-GRAS and its components was tested by Harrell's Concordance index (C-index) and Royston-Sauerbrei's R2D statistic.
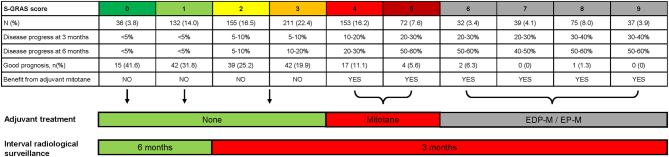
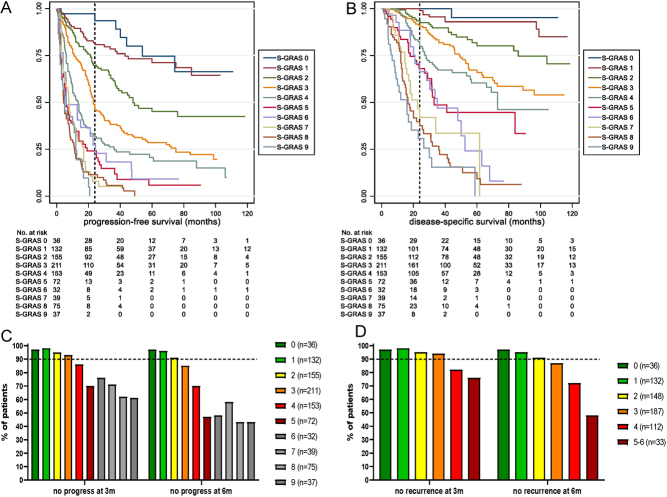
We included 942 ACC patients. The S-GRAS score showed superior prognostic performance for both PFS and DSS, with best discrimination obtained using the individual scores (0-9) (C-index = 0.73, R2D = 0.30, and C-index = 0.79, R2D = 0.45, respectively, all P < 0.01vs each component). The superiority of S-GRAS score remained when comparing patients treated or not with adjuvant mitotane (n = 481 vs 314). In particular, the risk of recurrence was significantly reduced as a result of adjuvant mitotane only in patients with S-GRAS 4-5.
The prognostic performance of S-GRAS is superior to tumour stage and Ki67 in operated ACC patients, independently from adjuvant mitotane. S-GRAS score provides a new important guide for personalised management of ACC (i.e. radiological surveillance and adjuvant treatment).
肾上腺皮质癌(ACC)具有侵袭性但临床表现多变。基于欧洲肾上腺肿瘤研究网络分期和 Ki67 指数的预后分层存在局限性。本研究旨在通过大型 ACC 患者队列证明基于积分的评分系统(S-GRAS)的预后作用。
这是一项多中心、回顾性 ACC 患者肾上腺切除术研究。
S-GRAS 评分通过以下积分相加计算:肿瘤分期(1-2=0;3=1;4=2)、分级(Ki67 指数 0-9%=0;10-19%=1;≥20%=2 分)、切除状态(R0=0;RX=1;R1=2;R2=3)、年龄(<50 岁=0;≥50 岁=1)、症状(无=0;有=1),以及分类,生成四个组(0-1、2-3、4-5 和 6-9)。终点为无进展生存期(PFS)和疾病特异性生存期(DSS)。S-GRAS 及其各组成部分的判别性能通过 Harrell 一致性指数(C 指数)和 Royston-Sauerbrei 的 R2D 统计量进行测试。
我们纳入了 942 例 ACC 患者。S-GRAS 评分对 PFS 和 DSS 具有更好的预后预测性能,使用单个评分(0-9)获得最佳区分度(C 指数=0.73,R2D=0.30;C 指数=0.79,R2D=0.45,均 P<0.01vs 每个组成部分)。在比较接受或不接受辅助米托坦治疗的患者(n=481 对 314)时,S-GRAS 评分的优势仍然存在。特别是,仅在 S-GRAS 4-5 患者中,辅助米托坦可显著降低复发风险。
S-GRAS 在接受手术的 ACC 患者中的预后预测性能优于肿瘤分期和 Ki67,与辅助米托坦无关。S-GRAS 评分可提供 ACC 患者个体化管理(即影像学监测和辅助治疗)的新重要指南。