Leukaemia Research Cytogenetics Group, Wolfson Childhood Cancer Research Centre, Clinical and Translational Research Institute, Newcastle University, Newcastle-upon-Tyne, UK.
Department of Haematology, Great Ormond Street Hospital, London, UK.
Lancet Haematol. 2021 Nov;8(11):e828-e839. doi: 10.1016/S2352-3026(21)00304-5.
High hyperdiploidy is the most common genetic subtype of childhood acute lymphoblastic leukaemia and is associated with a good outcome. However, some patients relapse and, given its prevalence, patients with high hyperdiploidy account for a large proportion of all relapses. We aimed to evaluate putative risk factors and determine the optimal pattern of trisomies for predicting outcome.
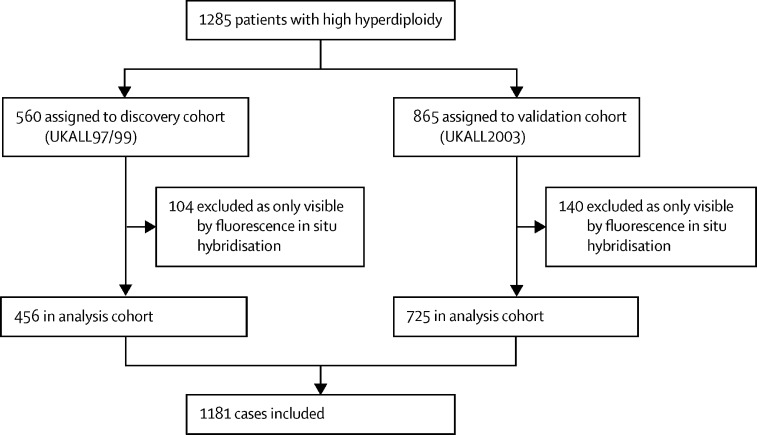
We used discovery and validation cohorts from consecutive trials-UKALL97/99 (n=456) and UKALL2003 (n=725)-to develop the prognostic profile. UKALL97/99 recruited patients aged 1-18 years between Jan 1, 1997, and June 15, 2002, and UKALL2003 recruited children and young adults aged 1-24 years between Oct 1, 2003, and June 30, 2001, from the UK and Ireland who were newly diagnosed with acute lymphoblastic leukaemia. Cytogenetic and fluorescence in-situ hybridisation testing was performed on pre-treatment bone marrow samples by regional UK National Health Service genetic laboratories or centrally by the Leukaemia Research Cytogenetics Group, and results were reported using established nomenclature and definitions. We examined the prognostic effect of previously proposed genetic and non-genetic risk factors among patients with high hyperdiploid acute lymphoblastic leukaemia treated on UKALL2003. We used Bayesian information criterion, targeted projection pursuit, and multivariate analysis to identify the optimal number of trisomies, and best subset regression and multivariate analysis to identify the optimal combination. Survival analysis considered three endpoints, as follows: event-free survival, defined as time to relapse, second tumour, or death, censored at last contact; relapse rate, defined as time to relapse for those reaching complete remission, censored at death in remission or last contact; and overall survival, defined as time to death, censored at last contact.
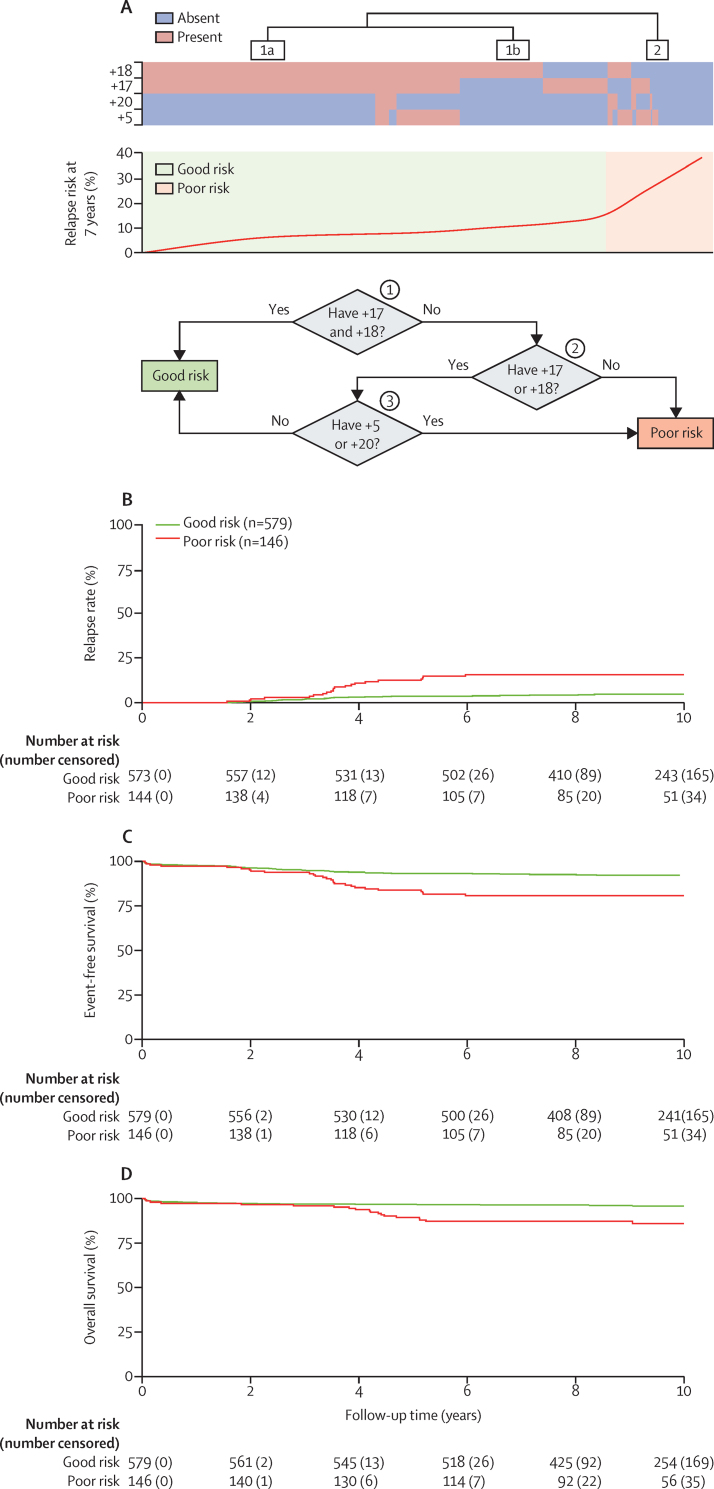
The median follow-up time for UKALL97/99 was 10·59 years (IQR 9·25-12·06) and 9·40 years (8·00-11·55) for UKALL2003. UKALL97/99 included 208 female patients and 248 male patients, and UKALL2003 included 345 female patients and 380 male patients. We deduced that the trisomic status of four chromosomes provided the optimal information for predicting outcome. The good risk profile comprised karyotypes with +17 and +18 or +17 or +18 in the absence of +5 and +20. All remaining cases were classified in the poor risk profile. The ratio of patients with good risk and poor risk was 82:18 and 80:20 in the discovery and validation cohorts, respectively. In the validation cohort, patients with the high hyperdiploid good risk profile had an improved response to treatment compared with other patients with high hyperdiploidy at 10 years (relapse rate 5% [95% CI 3-7] vs 16% [10-23]; p<0·0001; event-free survival 92% [90-94] vs 81% [73-86]; p<0·0001; and overall survival 96% [94-97] vs 86% [79-91]; p<0·0001). The outcome for high hyperdiploid poor risk patients was similar to that of patients with an intermediate cytogenetic profile. The prognostic effect of the UKALL high hyperdiploid profile was independent of minimal residual disease and the profile outperformed other high hyperdiploid risk profiles.
Future clinical trials and treatment protocols using high hyperdiploidy as a risk stratification factor should consider modifying the definition beyond chromosome count to incorporate this novel UKALL high hyperdiploid profile.
Blood Cancer UK.
高倍体性是儿童急性淋巴细胞白血病最常见的遗传亚型,与良好的预后相关。然而,一些患者会复发,鉴于其普遍性,高倍体性患者在所有复发患者中占很大比例。我们旨在评估潜在的危险因素,并确定最佳的三体模式来预测结果。
我们使用来自连续试验-UKALL97/99(n=456)和 UKALL2003(n=725)的发现和验证队列来开发预后特征。UKALL97/99 招募了 1997 年 1 月 1 日至 2002 年 6 月 15 日期间年龄在 1-18 岁之间的患者,UKALL2003 招募了 2003 年 10 月 1 日至 2001 年 6 月 30 日期间年龄在 1-24 岁之间的儿童和青年,来自英国和爱尔兰,他们新诊断为急性淋巴细胞白血病。通过区域英国国家卫生服务遗传实验室或由白血病研究细胞遗传学组集中对预处理骨髓样本进行细胞遗传学和荧光原位杂交检测,并使用既定的命名法和定义报告结果。我们检查了在 UKALL2003 中接受治疗的高倍体性急性淋巴细胞白血病患者中先前提出的遗传和非遗传危险因素的预后作用。我们使用贝叶斯信息准则、靶向投影追踪和多变量分析来确定最佳三体数量,并使用最佳子集回归和多变量分析来确定最佳组合。生存分析考虑了三个终点,如下所示:无事件生存,定义为复发、第二肿瘤或死亡的时间,截止到最后一次联系;复发率,定义为达到完全缓解的患者的复发时间,截止到缓解或最后一次联系时的死亡;总生存,定义为死亡时间,截止到最后一次联系。
UKALL97/99 的中位随访时间为 10.59 年(IQR 9.25-12.06),UKALL2003 的中位随访时间为 9.40 年(8.00-11.55)。UKALL97/99 包括 208 名女性患者和 248 名男性患者,UKALL2003 包括 345 名女性患者和 380 名男性患者。我们推断,四个染色体的三体状态为预测结果提供了最佳信息。良好的风险特征包括 +17 和 +18 或 +17 或 +18,而没有 +5 和 +20。所有其他病例均归类为不良风险特征。在发现队列和验证队列中,良好风险和不良风险的患者比例分别为 82:18 和 80:20。在验证队列中,与其他高倍体性患者相比,高倍体性良好风险患者的治疗反应更好,10 年时的复发率为 5%(95%CI 3-7)与 16%(10-23);p<0·0001;无事件生存率为 92%(90-94)与 81%(73-86);p<0·0001;总生存率为 96%(94-97)与 86%(79-91);p<0·0001)。高倍体性不良风险患者的预后与中间细胞遗传学特征患者相似。UKALL 高倍体性特征的预后作用独立于微小残留疾病,且该特征优于其他高倍体性风险特征。
未来使用高倍体性作为风险分层因素的临床试验和治疗方案应考虑在染色体计数之外修改定义,以纳入这一新的 UKALL 高倍体性特征。
英国血液癌症协会。