Ontario Health (Cancer Care Ontario), 525 University Ave, 3rd floor, Toronto, ON, M5G 2L3, Canada.
Canadian Centre for Applied Research in Cancer Control, 525 University Ave, 3rd floor, Toronto, ON, Canada.
BMC Cancer. 2021 Oct 29;21(1):1162. doi: 10.1186/s12885-021-08746-z.
While no direct comparative data exist for crizotinib in ROS1+ non-small cell lung cancer (NSCLC), studies have suggested clinical benefit with this targeted agent. The objective of this study was to assess the cost-effectiveness of crizotinib compared to standard platinum-doublet chemotherapy for first-line treatment of ROS1+ advanced NSCLC.
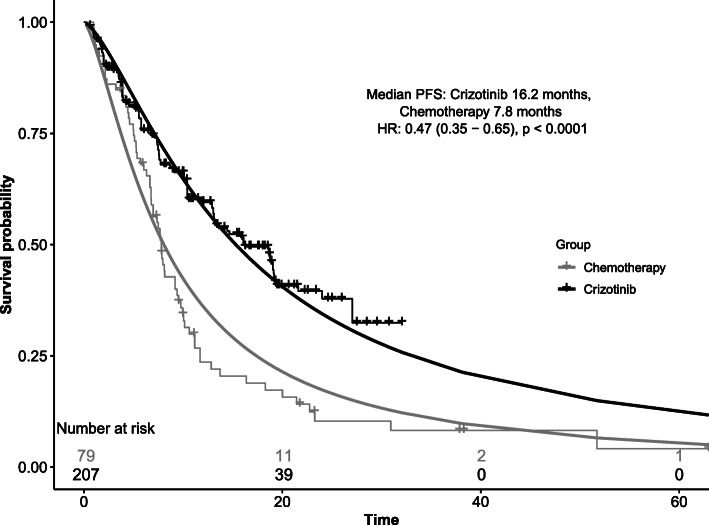
A Markov model was developed with a 10-year time horizon from the perspective of the Canadian publicly-funded health care system. Health states included progression-free survival (PFS), up to two further lines of therapy post-progression, palliation and death. Given a lack of comparative data and small study samples, crizotinib or chemotherapy studies with advanced ROS1+ NSCLC patients were identified and time-to-event data from digitized Kaplan-Meier curves were collected to pool PFS data. Costs of drugs, treatment administration, monitoring, adverse events and palliative care were included in 2018 Canadian dollars, with 1.5% discounting. An incremental cost-effectiveness ratio (ICER) was estimated probabilistically using 5000 simulations.
In the base-case probabilistic analysis, crizotinib produced additional 0.885 life-years and 0.772 quality-adjusted life-years (QALYs) at an incremental cost of $238,077, producing an ICER of $273,286/QALY gained. No simulations were found to be cost-effective at a willingness-to-pay threshold of $100,000/QALY gained. A scenario analysis assuming efficacy equivalent to the ALK+ NSCLC population showed a slightly more favorable cost-effectiveness profile for crizotinib.
Available data appear to support superior activity of crizotinib compared to chemotherapy in ROS1+ advanced NSCLC. At the list price, crizotinib was not cost-effective at commonly accepted willingness-to-pay thresholds across a wide range of sensitivity analyses.
虽然没有针对 ROS1+非小细胞肺癌(NSCLC)的克唑替尼直接比较数据,但研究表明该靶向药物具有临床获益。本研究旨在评估克唑替尼对比标准铂类双药化疗作为 ROS1+晚期 NSCLC 一线治疗的成本效果。
从加拿大公共卫生保健系统的角度出发,建立了一个具有 10 年时间范围的 Markov 模型。健康状态包括无进展生存期(PFS)、进展后进一步的二线治疗、姑息治疗和死亡。鉴于缺乏比较数据和小样本研究,确定了具有晚期 ROS1+ NSCLC 患者的克唑替尼或化疗研究,并收集数字化 Kaplan-Meier 曲线的时间事件数据以汇总 PFS 数据。药物、治疗管理、监测、不良事件和姑息治疗的成本均包含在 2018 年加拿大元中,并进行了 1.5%的贴现。使用 5000 次模拟进行了概率增量成本效果比(ICER)估计。
在基本案例概率分析中,克唑替尼在增加 0.885 个生命年和 0.772 个质量调整生命年(QALY)的情况下,额外增加了 238077 美元的增量成本,产生了 273286 美元/QALY 的增量成本效果比。在 100000 美元/QALY 获益的意愿支付阈值下,没有模拟结果被认为是具有成本效果的。在假设疗效与 ALK+ NSCLC 人群等效的情景分析中,克唑替尼的成本效果比略为有利。
现有数据似乎支持克唑替尼在 ROS1+晚期 NSCLC 中比化疗更有效。在现行价格下,在广泛的敏感性分析中,在普遍接受的意愿支付阈值内,克唑替尼并不具有成本效果。