Acute Cardiac Care Unit, Department of Cardiology, Hospital Universitario de Canarias, Ctra. La Cuesta-Taco, Ofra s/n, 38320 San Cristóbal de La Laguna, Tenerife, Spain.
Institut Municipal d'Investigacions Mèdiques (IMIM), Barcelona, Spain.
ESC Heart Fail. 2021 Dec;8(6):4820-4831. doi: 10.1002/ehf2.13670. Epub 2021 Oct 30.
The aim of the LAICA study was to evaluate the long-term effectiveness and safety of intermittent levosimendan infusion in patients with advanced heart failure (AdHF).
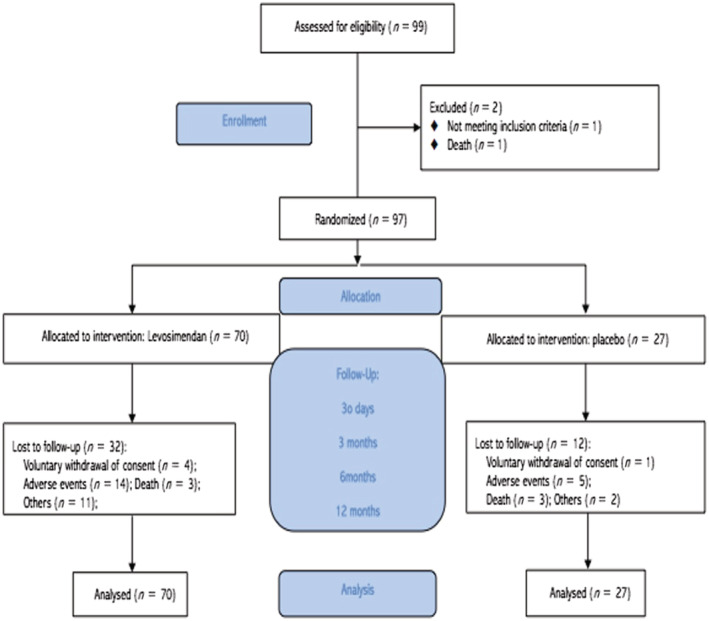
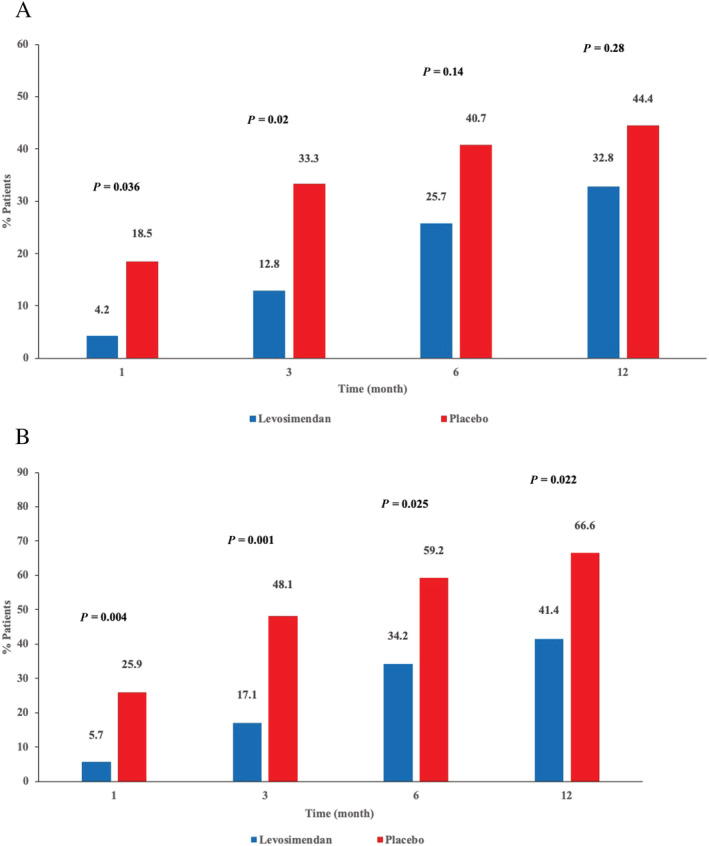
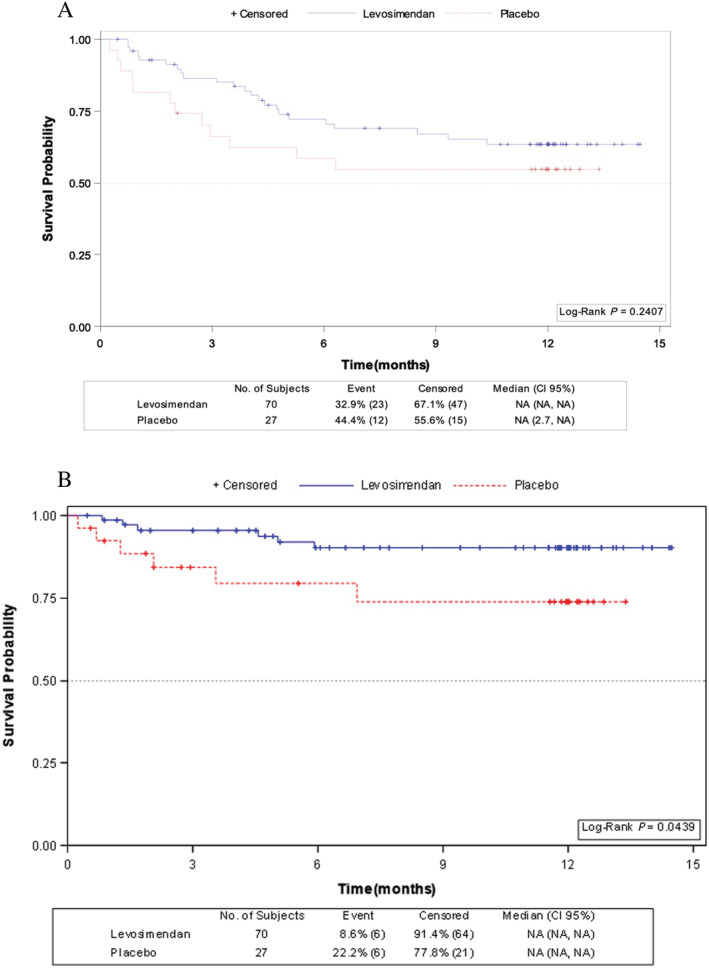
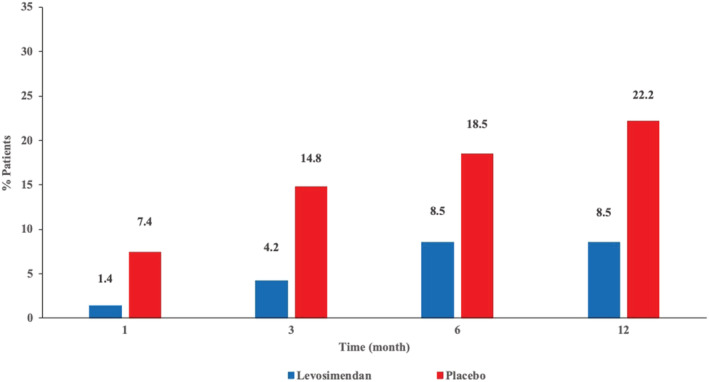
This was a multicentre, randomized, double-blind, placebo-controlled clinical trial of intermittent levosimendan 0.1 μg/kg/min as a continuous 24-h intravenous infusion administered once monthly for 1 year in patients with AdHF. The primary endpoint [incidence of rehospitalization (admission to the emergency department or hospital ward for >12 h) for acute decompensated HF or clinical deterioration of the underlying HF] occurred in 23/70 (33%) of the levosimendan group (Group I) and 12/27 (44%) of the placebo group (Group II) (P = 0.286). The incidence of hospital readmissions for acute decompensated HF (Group I vs. Group II) at 1, 3, 6, and 12 months was 4.2% vs. 18.2% (P = 0.036); 12.8% vs. 33.3% (P = 0.02); 25.7% vs. 40.7% (P = 0.147); 32.8% vs. 44.4% (P = 0.28), respectively. In a secondary pre-specified time-to-event analysis no differences were observed in admission for acute decompensated HF between patients treated with levosimendan compared with placebo (hazard ratio 0.66; 95% CI, 0.32-1.32; P = 0.24). Cumulative incidence for the aggregated endpoint of acute decompensation of HF and/or death at 1 and 3 months were significatively lower in the levosimendan group than in placebo group [5.7% vs. 25.9% (P = 0.004) and 17.1% vs. 48.1% (P = 0.001), respectively], but not at 6 and 12 months [34.2% vs. 59.2% (P = 0.025); 41.4% vs. 66.6% (P = 0.022), respectively]. Survival probability was significantly higher in patients who received levosimendan compared with those who received placebo (log rank: 4.06; P = 0.044). There were no clinically relevant differences in tolerability between levosimendan and placebo and no new safety signals were observed.
In our study, intermittent levosimendan in patients with AdHF produced a statistically non-significant reduction in the incidence of hospital readmissions for acute decompensated HF, a significantly lower cumulative incidence of acute decompensation of HF and/or death at 1 and 3 month of treatment and a significant improvement in survival during 12 months of treatment.
LAICA 研究的目的是评估晚期心力衰竭(AdHF)患者间歇性左西孟旦输注的长期有效性和安全性。
这是一项多中心、随机、双盲、安慰剂对照的临床试验,对 AdHF 患者进行为期 1 年的左西孟旦 0.1μg/kg/min 间歇性静脉滴注(每月 1 次,持续 24 小时)。主要终点[因急性失代偿性 HF 或基础 HF 病情恶化而再次住院(急诊或病房住院超过 12 小时)的发生率]发生在左西孟旦组(I 组)的 23/70(33%)和安慰剂组(II 组)的 12/27(44%)(P=0.286)。左西孟旦组(I 组)与安慰剂组(II 组)在 1、3、6 和 12 个月时因急性失代偿性 HF 而再次住院的发生率分别为 4.2%比 18.2%(P=0.036);12.8%比 33.3%(P=0.02);25.7%比 40.7%(P=0.147);32.8%比 44.4%(P=0.28)。在预先指定的二次时间事件分析中,与安慰剂相比,左西孟旦治疗患者因急性失代偿性 HF 入院的情况没有差异(风险比 0.66;95%CI,0.32-1.32;P=0.24)。左西孟旦组 1 个月和 3 个月时因急性 HF 失代偿和/或死亡的累积发生率显著低于安慰剂组[5.7%比 25.9%(P=0.004)和 17.1%比 48.1%(P=0.001)],但 6 个月和 12 个月时无差异[34.2%比 59.2%(P=0.025);41.4%比 66.6%(P=0.022)]。与接受安慰剂的患者相比,接受左西孟旦的患者的生存概率显著提高(对数秩检验:4.06;P=0.044)。左西孟旦和安慰剂的耐受性无临床相关差异,未观察到新的安全性信号。
在我们的研究中,晚期心力衰竭患者间歇性左西孟旦输注可降低因急性失代偿性 HF 再次住院的发生率,治疗 1 和 3 个月时因急性 HF 失代偿和/或死亡的累积发生率显著降低,12 个月时生存显著改善。