Rahimi Farzad, Vakhshoori Mehrbod, Heidarpour Maryam, Nouri Fatemeh, Heshmat-Ghahdarijani Kiyan, Fakhrolmobasheri Mohammad, Shafie Davood
Heart Failure Research Center, Cardiovascular Research Institute, Isfahan University of Medical Sciences, Isfahan, Iran.
Isfahan Endocrine and Metabolism Research Center, Isfahan University of Medical Sciences, Isfahan, Iran.
Crit Care Res Pract. 2021 Oct 22;2021:3820292. doi: 10.1155/2021/3820292. eCollection 2021.
One of the strategies for overcoming diuretic resistance among heart failure (HF) patients is adding thiazide-type diuretics. The main aim of this article is to compare the adverse clinical outcomes, including death and re-hospitalization, among individuals suffering from severe acute decompensated HF (ADHF) that consumed furosemide or furosemide plus metolazone.
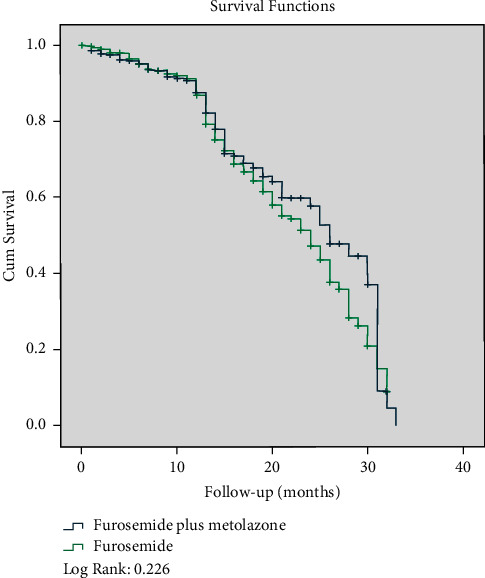
This retrospective cohort study was done in the context of the Persian registry of cardiovascular disease (PROVE) from September 2017 to September 2018. One thousand and four hundred thirty-eight individuals (furosemide: 972 and furosemide plus metolazone: 466) with the final diagnosis of severe ADHF (left ventricular ejection fraction < 30%) were selected and followed for 10.3 ± 7.8 months. The association between two groups, as mentioned above, with the incidence of death and re-admission, was evaluated with different models.
The mean age of the study population was 68.19 ± 12.98 years. There was no significant relation in terms of death or re-hospitalization between patients with different diuretic regimens. After adjustment of potential confounders, we found that adding metolazone as an adjuvant HF therapy was not independently associated with death or re-hospitalization (hazard ratio (HR): 0.78,95% confidence interval (CI) = 0.59-1.03, = 0.085, and odds ratio (OR): 0.80, 95% CI: 0.60-1.07, = 0.135, respectively).
Our findings revealed that adding metolazone in patients with furosemide resistance is not associated with higher morbidity and mortality. Therefore, usage of these two therapeutic agents could be a helpful strategy for severe HF patients.
在心力衰竭(HF)患者中克服利尿剂抵抗的策略之一是加用噻嗪类利尿剂。本文的主要目的是比较重度急性失代偿性心力衰竭(ADHF)患者中使用呋塞米或呋塞米加美托拉宗后的不良临床结局,包括死亡和再次住院情况。
这项回顾性队列研究于2017年9月至2018年9月在波斯心血管疾病登记处(PROVE)的背景下进行。选择了1438例最终诊断为重度ADHF(左心室射血分数<30%)的患者(呋塞米组:972例;呋塞米加美托拉宗组:466例),并随访10.3±7.8个月。使用不同模型评估上述两组与死亡和再次入院发生率之间的关联。
研究人群的平均年龄为68.19±12.98岁。不同利尿剂治疗方案的患者在死亡或再次住院方面无显著关联。在调整潜在混杂因素后,我们发现加用美托拉宗作为辅助性HF治疗与死亡或再次住院无独立关联(风险比(HR):0.78,95%置信区间(CI)=0.59 - 1.03,P = 0.085;优势比(OR):0.80,95% CI:0.60 - 1.07,P = 0.135)。
我们的研究结果表明,在呋塞米抵抗的患者中加用美托拉宗与更高的发病率和死亡率无关。因此,联合使用这两种治疗药物可能是重度HF患者的一种有用策略。