From the Service of Neurology (R.B.-V., R.A.D.P.), Department of Clinical Neurosciences, Lausanne University Hospital (Centre Hospitalier Universitaire Vaudois) and Lausanne University, Switzerland; Université Clermont Auvergne (X.M., P.C.), CHU de Clermont-Ferrand, Inserm, Neuro-Dol, ; Department of Neurology (N.M.), CHU de Poitiers, Hôpital La Milétrie; Department of Infectious Diseases (M.L., G.M.-B.), Toulouse University Hospital; Service de Neurologie, Pôle des Neurosciences Cliniques (J.-C.O.), CHU de Bordeaux Pellegrin Tripode; Service de Médecine Interne (M.R., B.G.), CHU Henri Mondor, Créteil; CRCSEP Nice (C.L.-F.), CHU de Nice, Université Nice Côte D'Azur, UR2CA-URRIS, Neurologie Pasteur 2; Department of Neurosciences (J.C.,D.B.), Toulouse University Hospital, France.
Neurol Neuroimmunol Neuroinflamm. 2021 Nov 2;9(1). doi: 10.1212/NXI.0000000000001097. Print 2022 Jan.
Progressive multifocal leukoencephalopathy (PML) is a disabling neurologic disorder resulting from the infection of the CNS by JC polyomavirus in immunocompromised individuals. For the last 2 decades, increasing use of immunotherapies leads to iatrogenic PML. Iatrogenic PML is often associated with signs of inflammation at onset (inflammatory PML) and/or after treatment withdrawal immune reconstitution inflammatory syndrome (PML-IRIS). Although immune reconstitution is a key element for viral clearance, it may also be harmful and induce clinical worsening. A C-C chemokine receptor type 5 (CCR5) antagonist (maraviroc) has been proposed to prevent and/or limit the deleterious immune responses underlying PML-IRIS. However, the data to support its use remain scarce and disputed.
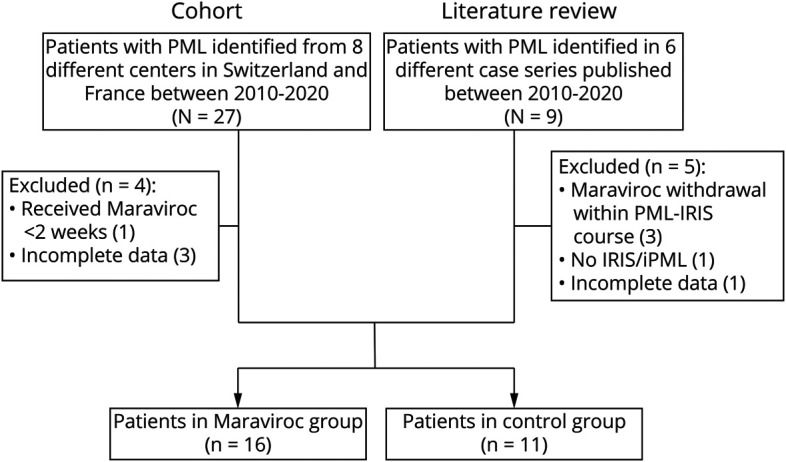
We conducted a multicenter retrospective cohort study at 8 university hospitals in France and Switzerland by collecting clinical, biological, and radiologic data of patients who developed inflammatory PML (iPML) or PML-IRIS related to immunosuppressive therapies used for chronic inflammatory diseases between 2010 and 2020. We added to this cohort, a meta-analysis of individual case reports of patients with iPML/PML-IRIS treated with maraviroc published up to 2021.
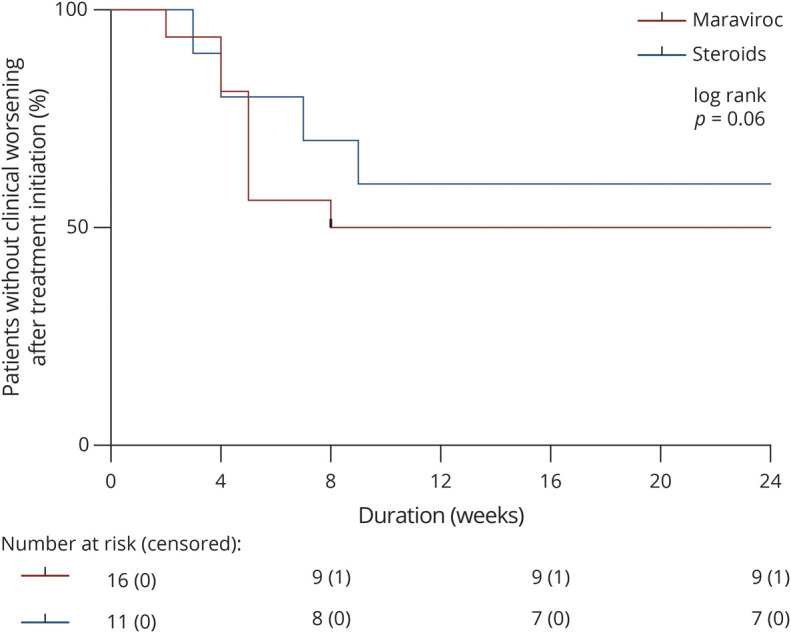
Overall, 27 cases were identified in the cohort and 9 from the literature. Among them, 27 met the inclusion criteria: 16 treated with maraviroc and 11 with standard of care (including corticosteroids use). Most cases were related to MS (92.6%) and natalizumab (88%). Inflammatory features (iPML) were present at onset in 12 patients (44.4%), and most patients (92.6%) received corticosteroids within the course of PML. Aggravation due to PML-IRIS was not prevented by maraviroc compared with patients who received only corticosteroids (adjusted odds ratio: 0.408, 95% CI: 0.06-2.63). Similarly, maraviroc did not influence time to clinical worsening due to PML-IRIS (adjusted hazard ratio = 0.529, 95% CI: 0.14-2.0) or disability at the last follow-up (adjusted odds ratio: 2, 95% CI: 0.23-17.3).
The use of CCR5 blockade did not help to keep deleterious immune reconstitution in check even when associated with corticosteroids. Despite maraviroc's reassuring safety profile, this study does not support its use in iPML/PML-IRIS.
This study provides Class IV evidence showing that adding maraviroc to the management of iatrogenic iPML/PML-IRIS does not improve the outcome.
进行性多灶性白质脑病(PML)是一种致残性的中枢神经系统疾病,由免疫抑制个体的 JC 多瘤病毒感染引起。在过去的 20 年中,免疫疗法的广泛应用导致了医源性 PML。医源性 PML 通常与发病时的炎症迹象(炎症性 PML)和/或治疗停止后的免疫重建炎症综合征(PML-IRIS)有关。尽管免疫重建是清除病毒的关键因素,但它也可能有害并导致临床恶化。一种 C-C 趋化因子受体 5(CCR5)拮抗剂(马拉维罗)已被提议用于预防和/或限制 PML-IRIS 潜在的有害免疫反应。然而,支持其使用的数据仍然很少且存在争议。
我们在法国和瑞士的 8 所大学医院进行了一项多中心回顾性队列研究,收集了 2010 年至 2020 年间因慢性炎症性疾病而接受免疫抑制治疗而发生炎症性 PML(iPML)或 PML-IRIS 的患者的临床、生物学和影像学数据。在此队列中,我们还增加了对截至 2021 年发表的接受马拉维罗治疗的 iPML/PML-IRIS 患者的个案报告的荟萃分析。
共在队列中发现 27 例,文献中发现 9 例。其中,27 例符合纳入标准:16 例接受马拉维罗治疗,11 例接受标准治疗(包括皮质类固醇治疗)。大多数病例与多发性硬化症(92.6%)和那他珠单抗(88%)有关。12 例患者(44.4%)在发病时存在炎症特征(iPML),大多数患者(92.6%)在 PML 病程中接受了皮质类固醇治疗。与仅接受皮质类固醇治疗的患者相比,马拉维罗并未预防 PML-IRIS 导致的恶化(调整后的优势比:0.408,95%CI:0.06-2.63)。同样,马拉维罗也没有影响因 PML-IRIS 而导致的临床恶化时间(调整后的危害比=0.529,95%CI:0.14-2.0)或最后一次随访时的残疾(调整后的优势比:2,95%CI:0.23-17.3)。
即使与皮质类固醇联合使用,CCR5 阻断也不能帮助控制有害的免疫重建。尽管马拉维罗具有可靠的安全性,但这项研究并不支持在 iPML/PML-IRIS 中使用它。
这项研究提供了 IV 级证据,表明在医源性 iPML/PML-IRIS 的治疗中添加马拉维罗并不能改善预后。