Brady Chloe A, Williams Charlotte, Batra Gauri, Church Elaine, Tower Clare L, Crocker Ian P, Heazell Alexander E P
Tommy's Maternal and Fetal Health Research Centre, St Mary's Hospital, The University of Manchester, Manchester, United Kingdom.
Exeter Medical School, University of Exeter, Exeter, United Kingdom.
Front Med (Lausanne). 2021 Oct 18;8:753220. doi: 10.3389/fmed.2021.753220. eCollection 2021.
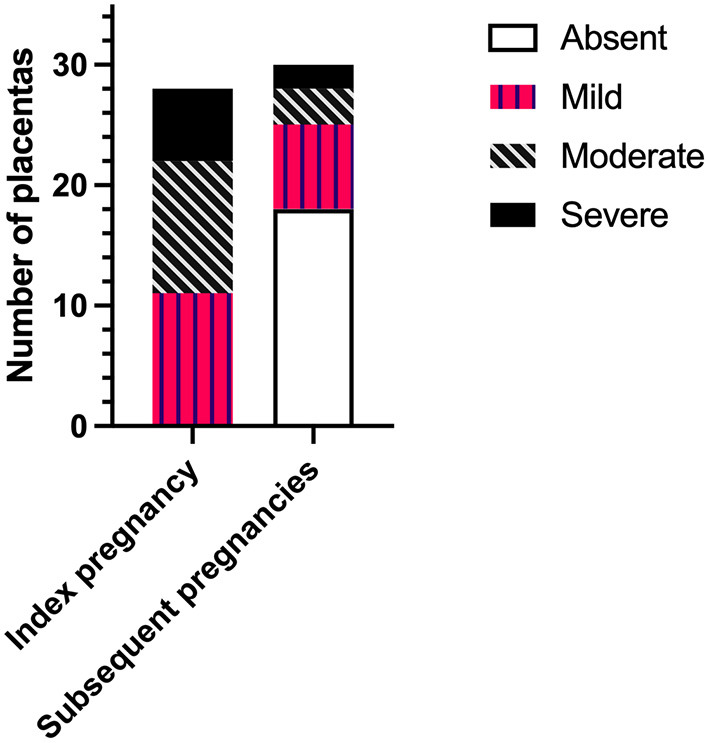
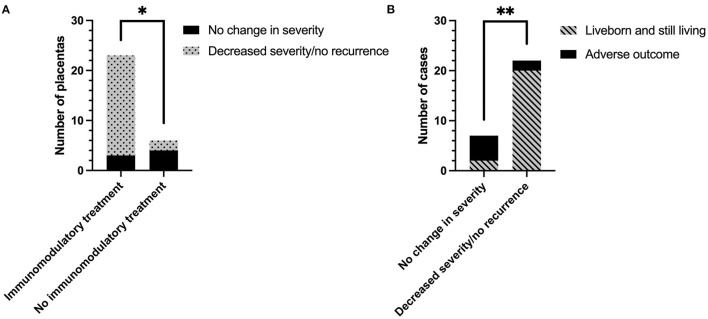
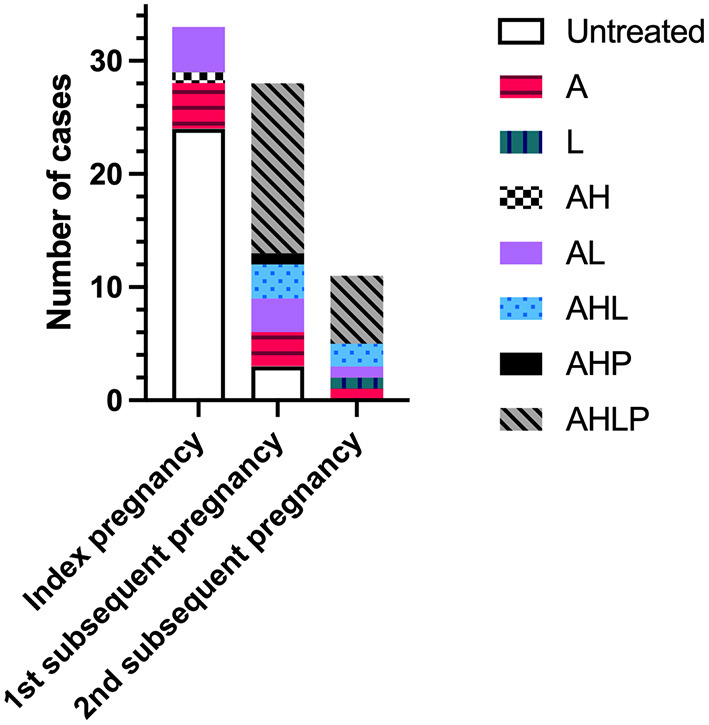
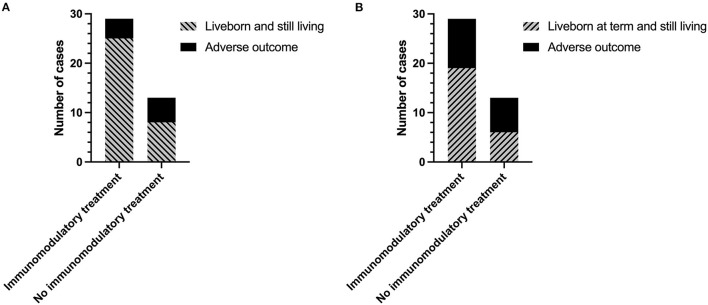
Chronic histiocytic intervillositis (CHI) is a rare, but highly recurrent inflammatory placental lesion wherein maternal macrophages infiltrate the intervillous space. Pregnancies with CHI are at high risk of fetal growth restriction, miscarriage or stillbirth. Presently, the diagnosis can only be made after histopathological examination of the placenta. Given its proposed immunological etiology, current treatments include aspirin, heparin, and immunomodulatory agents. However, the rationale for these medications is largely based upon small case series and reports as there is a lack of larger studies investigating treatment efficacy. Therefore, this study sought to determine whether inclusion of immunomodulatory medications was effective at reducing the severity of lesions and improving pregnancy outcomes in subsequent pregnancies. Thirty-three women with a history of CHI in at least one pregnancy (index case) were identified retrospectively through medical records. Twenty-eight participants presented with a first subsequent pregnancy and a further 11 with a second subsequent pregnancy at a specialist clinic for pregnancy after loss. Data on maternal demographics, medical history, medication, pregnancy outcome, and placental pathology was collected and compared between pregnancies. Twenty-seven (69%) subsequent pregnancies were treated with at least one or both of prednisolone and hydroxychloroquine. Inclusion of at least one immunomodulatory agent in treatment regimen resulted in an almost 25% increase in overall livebirth rate (61.5 vs. 86.2%). In women treated with immunomodulatory medication a greater proportion of placentas had reduced severity of lesions compared to those treated without (86.7 vs. 33.3%, respectively). A reduction in CHI severity was associated with a 62.3% improvement in livebirth rate compared to those where severity remained unchanged in relation to the index case. These data provide preliminary evidence that the use of immunomodulatory medication in the management of CHI improves histopathological lesions and the chance of livebirth in subsequent pregnancies. Due to CHI's rarity and ethical and feasibility issues, randomized controlled trials in affected women are challenging to conduct. As a result, collaboration between centers is required in future to increase study sample sizes and elucidate the mechanisms of hydroxychloroquine and prednisolone in reducing pathology.
慢性组织细胞性绒毛间炎(CHI)是一种罕见但复发率很高的胎盘炎症性病变,母体巨噬细胞会浸润绒毛间隙。患有CHI的孕妇面临胎儿生长受限、流产或死产的高风险。目前,只有在对胎盘进行组织病理学检查后才能做出诊断。鉴于其推测的免疫病因,目前的治疗方法包括阿司匹林、肝素和免疫调节药物。然而,这些药物的使用依据主要基于小病例系列和报告,因为缺乏关于治疗效果的大型研究。因此,本研究旨在确定使用免疫调节药物是否能有效降低病变严重程度并改善后续妊娠的结局。通过病历回顾性确定了33名至少有一次妊娠史(索引病例)的CHI女性。28名参与者迎来了首次后续妊娠,另有11名在一家专门的流产后妊娠诊所迎来了第二次后续妊娠。收集并比较了各次妊娠之间的产妇人口统计学、病史、用药情况、妊娠结局和胎盘病理学数据。27例(69%)后续妊娠接受了泼尼松龙和羟氯喹中的至少一种或两种药物治疗。治疗方案中加入至少一种免疫调节药物使总体活产率提高了近25%(61.5%对86.2%)。与未接受免疫调节药物治疗的女性相比,接受免疫调节药物治疗的女性中,胎盘病变严重程度降低的比例更高(分别为86.7%对33.3%)。与索引病例相比,CHI严重程度降低的患者活产率提高了62.3%。这些数据提供了初步证据,表明在CHI的管理中使用免疫调节药物可改善组织病理学病变,并增加后续妊娠的活产机会。由于CHI罕见以及伦理和可行性问题,对受影响女性进行随机对照试验具有挑战性。因此,未来需要各中心之间开展合作,以增加研究样本量,并阐明羟氯喹和泼尼松龙在减轻病变方面的机制。