Department of Medicine, Duke University School of Medicine, Durham, North Carolina.
Health Services Research and Development Center of Innovation, Durham Veterans Affairs Health Care System, Durham, North Carolina.
JAMA Netw Open. 2021 Nov 1;4(11):e2133188. doi: 10.1001/jamanetworkopen.2021.33188.
One-third of US residents have trouble paying their medical bills. They often turn to their physicians for help navigating health costs and insurance coverage.
To determine whether physicians can accurately estimate out-of-pocket expenses when they are given all of the necessary information about a drug's price and a patient's insurance plan.
DESIGN, SETTING, AND PARTICIPANTS: This national mail-in survey used a random sample of US physicians. The survey was sent to 900 outpatient physicians (300 each of primary care, gastroenterology, and rheumatology). Physicians were excluded if they were in training, worked primarily for the Veterans Administration or Indian Health Service, were retired, or reported 0% outpatient clinical effort. Analyses were performed from July to December 2020.
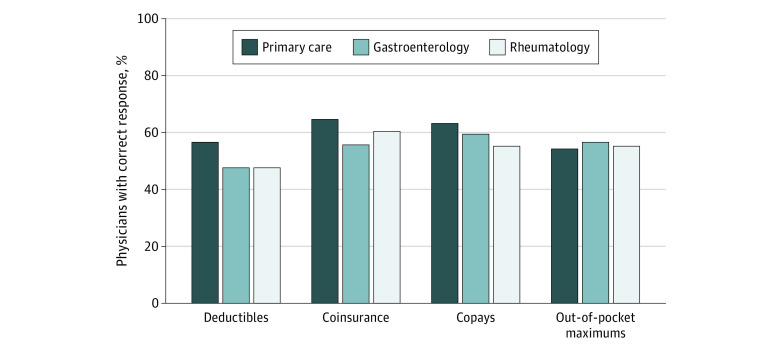
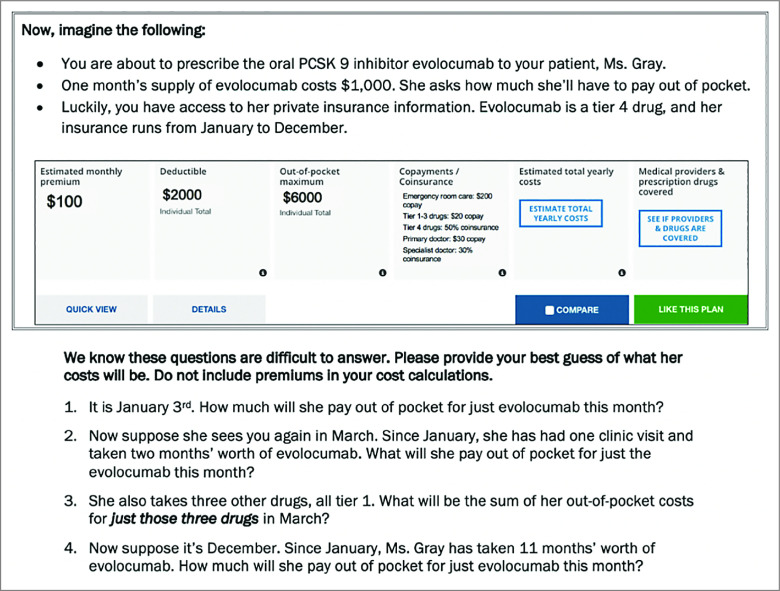
In a hypothetical vignette, a patient was prescribed a new drug costing $1000/month without insurance. A summary of her private insurance information was provided, including the plan's deductible, coinsurance rates, copays, and out-of-pocket maximum. Physicians were asked to estimate the drug's out-of-pocket cost at 4 time points between January and December, using the plan's 4 types of cost-sharing: (1) deductibles, (2) coinsurance, (3) copays, and (4) out-of-pocket maximums. Multivariate linear regression was used to assess differences in performance by specialty, adjusting for attitudes toward cost conversations, demographics, and clinical characteristics.
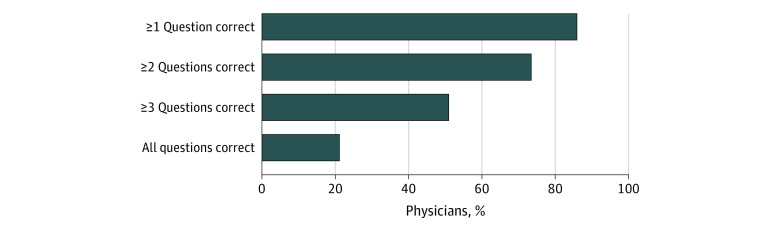
The response rate was 45% (405 of 900) and 371 respondents met inclusion criteria. Among the respondents included in this study, 59% (n = 220) identified as male, 23% (n = 84) as Asian, 3% (n = 12) as Black, 6% (n = 24) as Hispanic, and 58% (n = 216) as White; 30% (n = 112) were primary care physicians, 35% (n = 128) were gastroenterologists, and 35% (n = 131) were rheumatologists; and the mean (SD) age was 49 (10) years. Overall, 52% of physicians (n = 192) accurately estimated costs before the deductible was met, 62% (n = 228) accurately used coinsurance information, 61% (n = 224) accurately used copay information, and 57% (n = 210) accurately estimated costs once the out-of-pocket maximum was met. Only 21% (n = 78) of physicians answered all 4 questions correctly. Ability to estimate out-of-pocket costs was not associated with specialty, attitudes toward cost conversations, or clinic characteristics.
This survey study found that many US physicians have difficulty estimating out-of-pocket costs, even when they have access to their patients' insurance plans. The mechanics involved in calculating real-time out-of-pocket costs are complex. These findings suggest that increased price transparency and simpler insurance cost-sharing mechanisms are needed to enable informed cost conversations at the point of prescribing.
三分之一的美国居民在支付医疗费用方面有困难。他们经常向医生寻求帮助,以了解健康费用和保险覆盖范围。
确定当医生获得有关药物价格和患者保险计划的所有必要信息时,他们是否可以准确估算自付费用。
设计、设置和参与者:这项全国性的邮件调查使用了美国医生的随机样本。该调查寄给了 900 名门诊医生(每组 300 名,分别为初级保健医生、胃肠病学家和风湿病学家)。如果医生正在接受培训、主要为退伍军人管理局或印度卫生服务局工作、退休或报告门诊临床工作为 0%,则将其排除在外。分析于 2020 年 7 月至 12 月进行。
在一个假设的情景中,为一名没有保险的患者开了一种新的每月花费 1000 美元的药物。提供了她私人保险信息的摘要,包括计划的免赔额、共同保险费率、共同支付额和自付额上限。医生被要求在 1 月至 12 月的 4 个时间点使用计划的 4 种费用分担类型(1)免赔额、(2)共同保险、(3)共同支付额和(4)自付额上限来估算药物的自付费用。使用多元线性回归来评估专业差异对表现的影响,调整了对成本对话的态度、人口统计学和临床特征。
回应率为 45%(900 名中的 405 名),符合纳入标准的有 371 名应答者。在本研究中包括的应答者中,59%(n=220)为男性,23%(n=84)为亚洲人,3%(n=12)为黑人,6%(n=24)为西班牙裔,58%(n=216)为白人;30%(n=112)为初级保健医生,35%(n=128)为胃肠病学家,35%(n=131)为风湿病学家;平均(SD)年龄为 49(10)岁。总体而言,52%的医生(n=192)在免赔额达到之前准确估算了费用,62%(n=228)准确使用了共同保险信息,61%(n=224)准确使用了共同支付信息,57%(n=210)准确估算了自付额上限达到后的费用。只有 21%(n=78)的医生正确回答了所有 4 个问题。估算自付费用的能力与专业、对成本对话的态度或诊所特征无关。
这项调查研究发现,即使美国医生可以访问患者的保险计划,许多医生在估算自付费用方面也存在困难。计算实时自付费用的机制非常复杂。这些发现表明,需要增加价格透明度和更简单的保险成本分担机制,以便在开处方时进行知情的成本对话。