National Heart Centre Singapore & Duke-National University of Singapore Singapore.
Duke Clinical Research InstituteDuke University School of Medicine Durham NC.
J Am Heart Assoc. 2021 Nov 16;10(22):e021094. doi: 10.1161/JAHA.121.021094. Epub 2021 Nov 6.
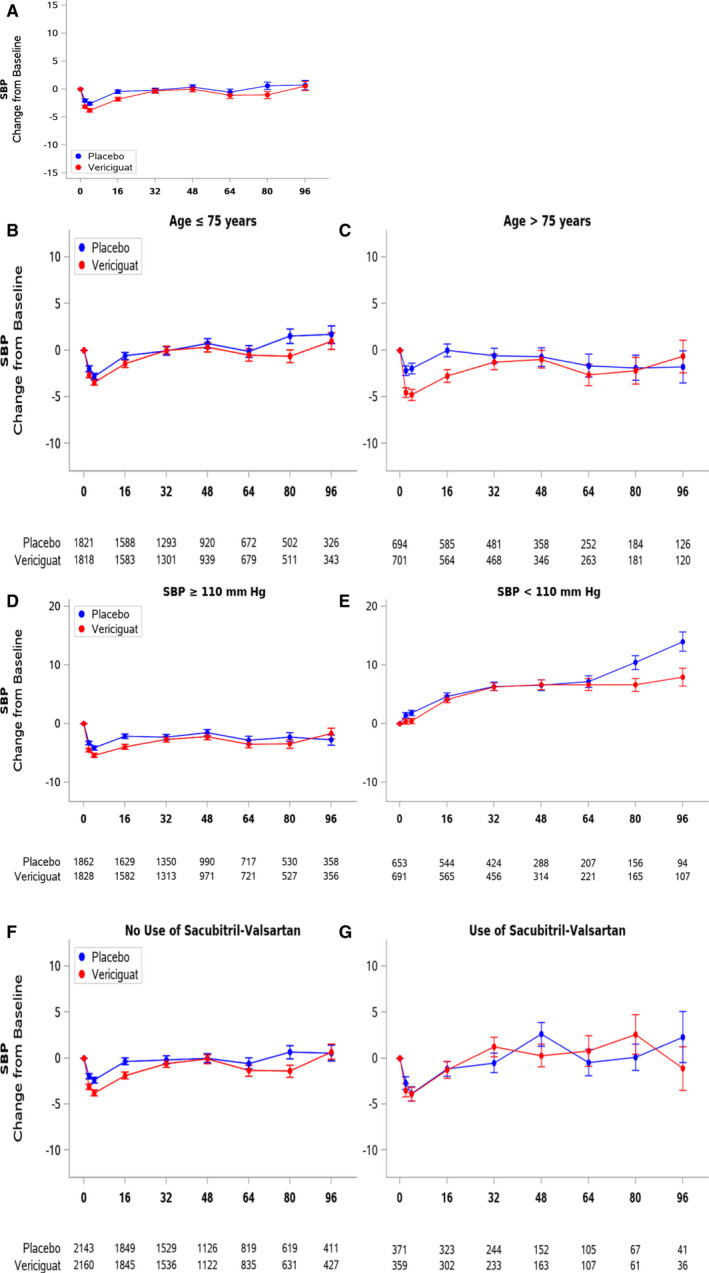
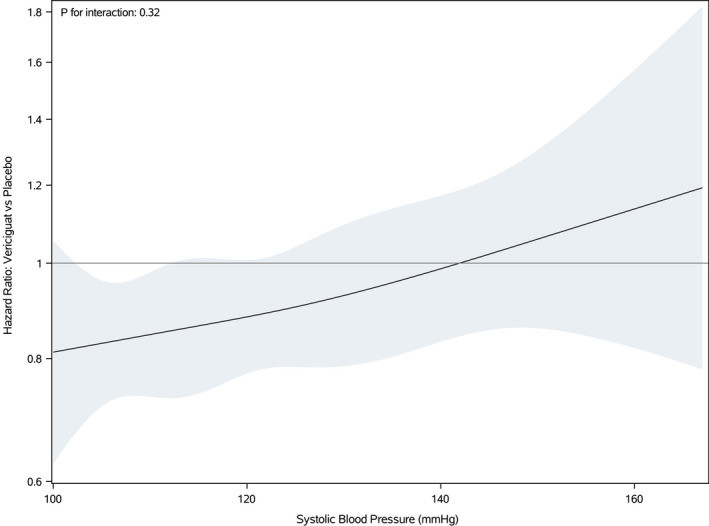
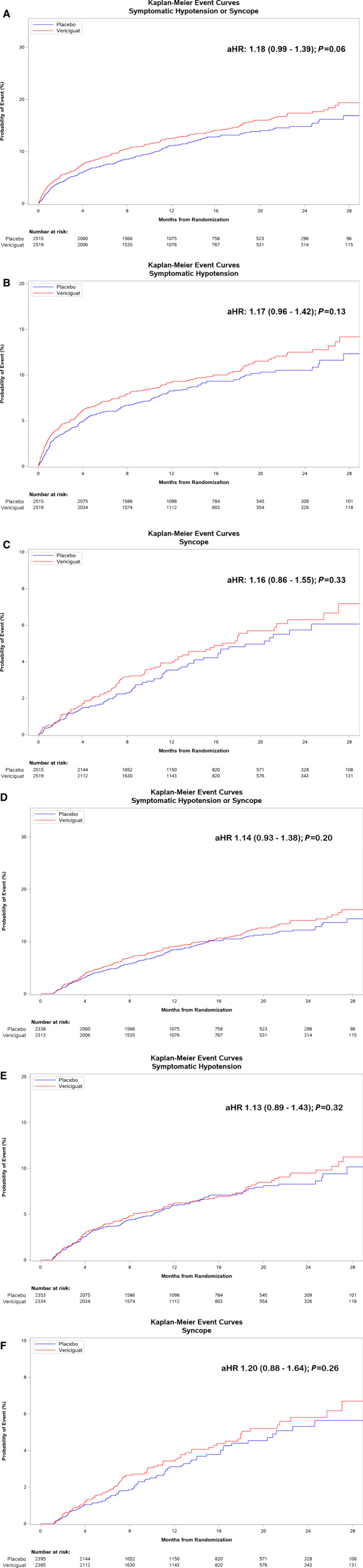
Background Although safety and tolerability of vericiguat were established in the VICTORIA (Vericiguat Global Study in Subjects With Heart Failure With Reduced Ejection Fraction) trial in patients with heart failure with reduced ejection fraction, some subgroups may be more susceptible to symptomatic hypotension, such as older patients, those with lower baseline systolic blood pressure (SBP), or those concurrently taking angiotensin receptor neprilysin inhibitors. We described the SBP trajectories over time and compared the occurrence of symptomatic hypotension or syncope by treatment arm in potentially vulnerable subgroups in VICTORIA. We also evaluated the relation between the efficacy of vericiguat and baseline SBP. Methods and Results Among patients receiving at least 1 dose of the study drug (n=5034), potentially vulnerable subgroups were those >75 years old (n=1395), those with baseline SBP 100-110 mm Hg (n=1344), and those taking angiotensin receptor neprilysin inhibitors (n=730). SBP trajectory was plotted as mean change from baseline over time. The treatment effect on time to symptomatic hypotension or syncope was evaluated overall and by subgroup, and the primary efficacy composite outcome (heart failure hospitalization or cardiovascular death) across baseline SBP was examined using Cox proportional hazards models. SBP trajectories showed a small initial decline in SBP with vericiguat in those >75 years old (versus younger patients), as well as those receiving angiotensin receptor neprilysin inhibitors (versus none), with SBP returning to baseline thereafter. Patients with SBP <110 mm Hg at baseline showed a trend to increasing SBP over time, which was similar in both treatment arms. Safety event rates were generally low and similar between treatment arms within each subgroup. In Cox proportional hazards analysis, there were similar numbers of safety events with vericiguat versus placebo (adjusted hazard ratio [HR], 1.18; 95% CI, 0.99-1.39; =0.059). No difference existed between treatment arms in landmark analysis beginning after the titration phase (ie, post 4 weeks) (adjusted HR, 1.14; 95% CI, 0.93-1.38; =0.20). The benefit of vericiguat compared with placebo on the primary composite efficacy outcome was similar across the spectrum of baseline SBP ( for interaction=0.32). Conclusions These data demonstrate the safety of vericiguat in a broad population of patients with worsening heart failure with reduced ejection fraction, even among those predisposed to hypotension. Vericiguat's efficacy persisted regardless of baseline SBP. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT02861534.
背景 尽管在射血分数降低的心力衰竭患者中进行的 VICTORIA(Vericiguat 全球研究在射血分数降低的心力衰竭患者中的研究)试验已经证实了维立西呱的安全性和耐受性,但某些亚组可能更容易出现有症状的低血压,例如老年患者、基线收缩压(SBP)较低的患者或同时服用血管紧张素受体脑啡肽酶抑制剂的患者。我们描述了 VICTORIA 中潜在脆弱亚组随时间推移的 SBP 轨迹,并按治疗组比较了有症状的低血压或晕厥的发生情况。我们还评估了维立西呱的疗效与基线 SBP 之间的关系。
方法和结果 在接受至少一剂研究药物的患者中(n=5034),潜在脆弱亚组包括年龄>75 岁的患者(n=1395)、基线 SBP 为 100-110mmHg 的患者(n=1344)和服用血管紧张素受体脑啡肽酶抑制剂的患者(n=730)。SBP 轨迹作为随时间从基线的平均变化绘制。总体上和按亚组评估了治疗对有症状的低血压或晕厥发生时间的影响,并使用 Cox 比例风险模型检查了整个基线 SBP 上的主要疗效复合结局(心力衰竭住院或心血管死亡)。SBP 轨迹显示,与年轻患者相比,年龄>75 岁的患者(与年轻患者相比)以及接受血管紧张素受体脑啡肽酶抑制剂的患者(与未接受患者相比)的 SBP 在使用维立西呱后初期略有下降,此后 SBP 恢复至基线。基线 SBP<110mmHg 的患者随时间呈现 SBP 升高的趋势,在两个治疗组中均相似。安全性事件发生率通常较低,并且在每个亚组内的治疗组之间相似。在 Cox 比例风险分析中,维立西呱与安慰剂相比,安全性事件的数量相似(调整后的危险比[HR],1.18;95%CI,0.99-1.39;=0.059)。在从滴定阶段(即 4 周后)开始的标志性分析中,治疗组之间没有差异(调整后的 HR,1.14;95%CI,0.93-1.38;=0.20)。与安慰剂相比,维立西呱在整个基线 SBP 范围内(交互项=0.32)的主要复合疗效结局均具有相似的获益。
结论 这些数据表明,维立西呱在射血分数降低的心力衰竭恶化的广泛患者人群中是安全的,即使在易发生低血压的患者中也是如此。无论基线 SBP 如何,维立西呱的疗效均保持不变。