Resuscitation InstituteRosalind Franklin University of Medicine and Science North Chicago IL.
Section of Critical Care MedicineCAPT James A. Lovell Federal Health Care Center North Chicago IL.
J Am Heart Assoc. 2021 Dec 7;10(23):e023956. doi: 10.1161/JAHA.121.023956. Epub 2021 Nov 8.
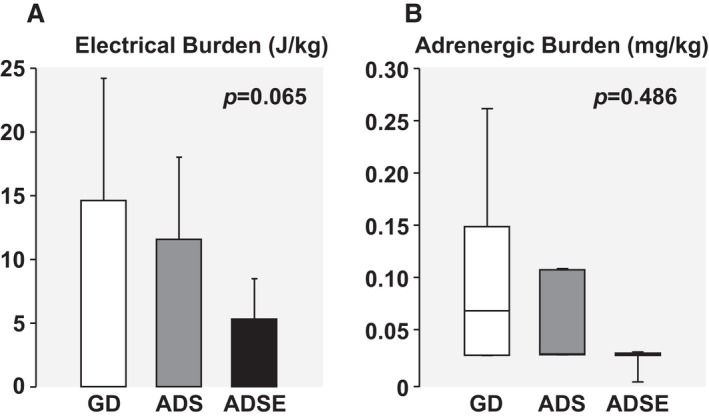
Background We previously reported that resuscitation delivering electrical shocks guided by real-time ventricular fibrillation amplitude spectral area (AMSA) enabled return of spontaneous circulation (ROSC) with fewer shocks, resulting in less myocardial dysfunction. We now hypothesized that AMSA could also guide delivery of epinephrine, expecting further outcome improvement consequent to less electrical and adrenergic burdens. Methods and Results A swine model of ventricular fibrillation was used to compare after 10 minutes of untreated ventricular fibrillation a guidelines-driven (n=8) resuscitation protocol, delivering shocks every 2 minutes and epinephrine every 4 minutes, with an AMSA-driven shocks (n=8) protocol, delivering epinephrine every 4 minutes, and with an AMSA-driven shocks and epinephrine (ADSE; n=8) protocol. For guidelines-driven, AMSA-driven shocks, and ADSE protocols, the time to ROSC (mean±SD) was 569±164, 410±111, and 400±80 seconds (=0.045); the number of shocks (mean±SD) was 5±2, 3±1, and 3±2 (=0.024) with ADSE fewer than guidelines-driven (=0.03); and the doses of epinephrine (median [interquartile range]) were 2.0 (1.3-3.0), 1.0 (1.0-2.8), and 1.0 (0.3-3.0) (=0.419). The ROSC rate was similar, yet survival after ROSC favored AMSA-driven protocols (guidelines-driven, 3/6; AMSA-driven shocks, 6/6; and ADSE, 7/7; =0.019 by log-rank test). Left ventricular function and survival after ROSC correlated inversely with electrical burden (ie, cumulative unsuccessful shocks, J/kg; =0.020 and =0.046) and adrenergic burden (ie, total epinephrine doses, mg/kg; =0.042 and =0.002). Conclusions Despite similar ROSC rates achieved with all 3 protocols, AMSA-driven shocks and ADSE resulted in less postresuscitation myocardial dysfunction and better survival, attributed to attaining ROSC with less electrical and adrenergic myocardial burdens.
背景 我们之前的研究表明,实时心室颤动幅度谱面积(AMSA)指导的除颤可以恢复自主循环(ROSC),所需电击次数更少,导致心肌功能障碍更少。我们现在假设 AMSA 也可以指导肾上腺素的输送,预计电击和肾上腺素的负担减少会带来进一步的改善。 方法和结果 我们使用猪心室颤动模型比较了 10 分钟未治疗的心室颤动后,采用指南指导(n=8)的复苏方案,每 2 分钟给予电击,每 4 分钟给予肾上腺素,采用 AMSA 驱动的电击(n=8)方案,每 4 分钟给予肾上腺素,以及采用 AMSA 驱动的电击和肾上腺素(ADSE;n=8)方案。对于指南驱动、AMSA 驱动电击和 ADSE 方案,ROSC 的时间(平均值±SD)分别为 569±164、410±111 和 400±80 秒(=0.045);电击次数(平均值±SD)分别为 5±2、3±1 和 3±2(=0.024),ADSE 比指南驱动少(=0.03);肾上腺素剂量(中位数[四分位距])分别为 2.0(1.3-3.0)、1.0(1.0-2.8)和 1.0(0.3-3.0)(=0.419)。ROSC 率相似,但 ROSC 后的存活率有利于 AMSA 驱动的方案(指南驱动,3/6;AMSA 驱动电击,6/6;ADSE,7/7;=0.019,对数秩检验)。左心室功能和 ROSC 后的存活率与电负荷(即累积未成功电击次数,J/kg;=0.020 和=0.046)和肾上腺素负荷(即总肾上腺素剂量,mg/kg;=0.042 和=0.002)呈负相关。 结论 尽管所有 3 种方案的 ROSC 率相似,但 AMSA 驱动电击和 ADSE 导致复苏后心肌功能障碍更小、存活率更高,这归因于用更少的电和肾上腺素心肌负荷实现 ROSC。