Department of Cardiothoracic Surgery, Leiden University Medical Center, Leiden, Netherlands.
Department of Cardiology, Biomechanical Engineering, Erasmus MC, Rotterdam, Netherlands.
Eur J Cardiothorac Surg. 2022 Jun 15;62(1). doi: 10.1093/ejcts/ezab478.
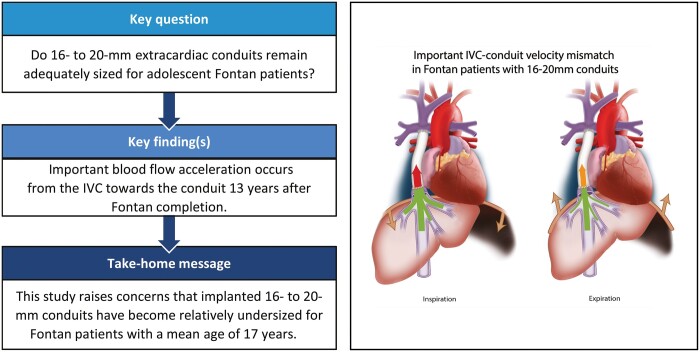
Adequacy of 16-20mm extracardiac conduits for adolescent Fontan patients remains unknown. This study aims to evaluate conduit adequacy using the inferior vena cava (IVC)-conduit velocity mismatch factor along the respiratory cycle.
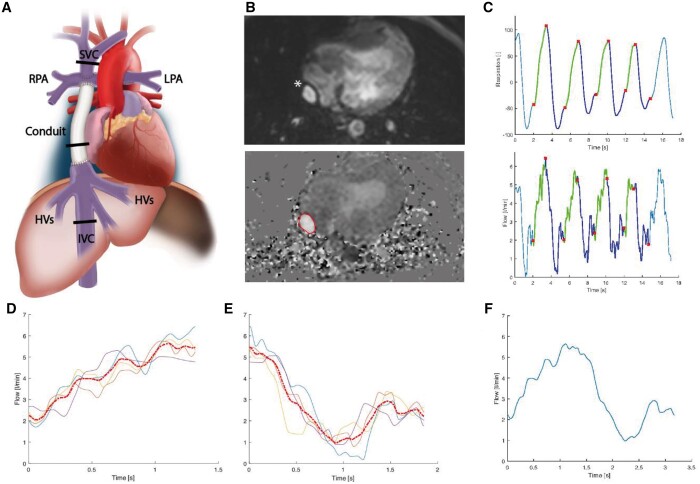
Real-time 2D flow MRI was prospectively acquired in 50 extracardiac (16-20mm conduits) Fontan patients (mean age 16.9 ± 4.5 years) at the subhepatic IVC, conduit and superior vena cava. Hepatic venous flow was determined by subtracting IVC flow from conduit flow. The cross-sectional area (CSA) was reported for each vessel. Mean flow and velocity was calculated during the average respiratory cycle, inspiration and expiration. The IVC-conduit velocity mismatch factor was determined as follows: Vconduit/VIVC, where V is the mean velocity.
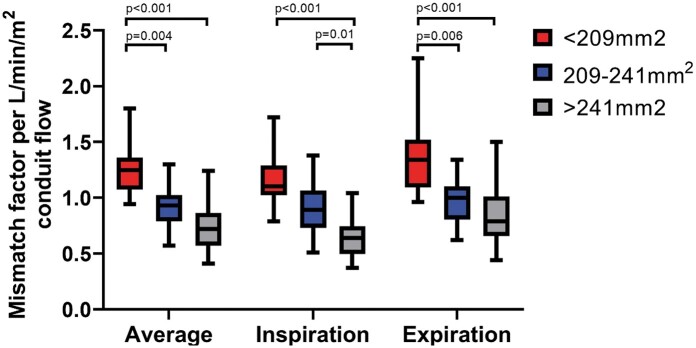
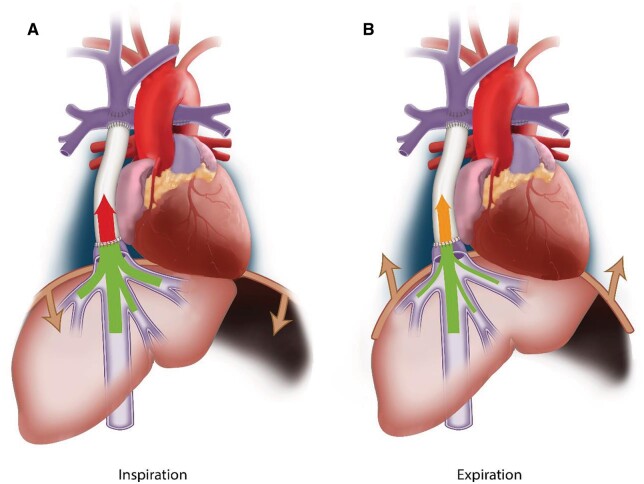
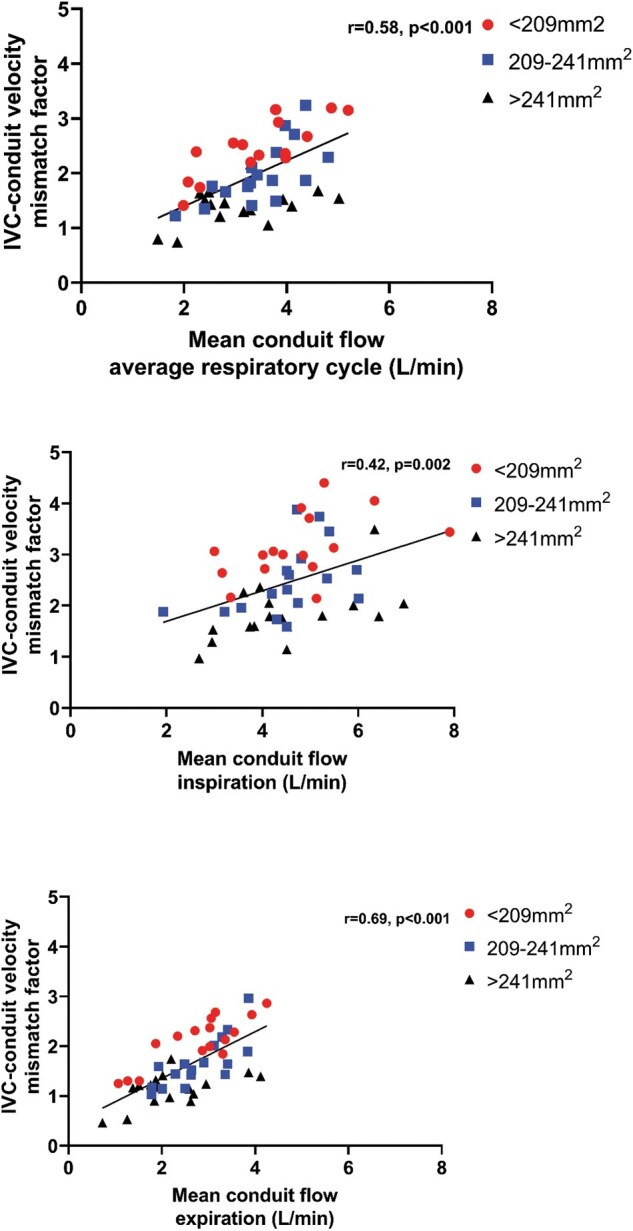
Median conduit CSA and IVC CSA were 221 mm2 (Q1-Q3 201-255) and 244 mm2 (Q1-Q3 203-265), respectively. From the IVC towards the conduit, flow rates increased significantly due to the entry of hepatic venous flow (IVC 1.9, Q1-Q3 1.5-2.2) versus conduit (3.3, Q1-Q3 2.5-4.0 l/min, P < 0.001). Consequently, mean velocity significantly increased (IVC 12 (Q1-Q3 11-14 cm/s) versus conduit 25 (Q1-Q3 17-31 cm/s), P < 0.001), resulting in a median IVC-conduit velocity mismatch of 1.8 (Q1-Q3 1.5-2.4), further augmenting during inspiration (median 2.3, Q1-Q3 1.8-3.0). IVC-conduit mismatch was inversely related to measured conduit size and positively correlated with conduit flow. The normalized IVC-conduit velocity mismatch factor during expiration and the entire respiratory cycle correlated with peak VO2 (r = -0.37, P = 0.014 and r = -0.31, P = 0.04, respectively).
Important blood flow accelerations are observed from the IVC towards the conduit in adolescent Fontan patients, which is related to peak VO2. This study, therefore, raises concerns that implanted 16-20mm conduits have become undersized for older Fontan patients and future studies should clarify its effect on long-term outcome.
目前尚不清楚 16-20mm 心外管道在青少年 Fontan 患者中的充分性。本研究旨在通过下腔静脉(IVC)-导管速度在呼吸周期中的不匹配因子来评估导管的充分性。
前瞻性地在 50 例(16-20mm 心外导管)Fontan 患者(平均年龄 16.9±4.5 岁)的肝下 IVC、导管和上腔静脉(SVC)中采集实时二维流动 MRI。通过从导管流量中减去 IVC 流量来确定肝静脉流量。报告了每个血管的横截面积(CSA)。在平均呼吸周期、吸气和呼气期间计算平均流量和速度。IVC-导管速度不匹配因子如下确定:V 导管/VIVC,其中 V 是平均速度。
导管 CSA 和 IVC CSA 的中位数分别为 221mm2(Q1-Q3 201-255)和 244mm2(Q1-Q3 203-265)。从 IVC 到导管,由于肝静脉血流的流入,流量率显著增加(IVC 为 1.9,Q1-Q3 为 1.5-2.2)与导管(3.3,Q1-Q3 为 2.5-4.0 l/min,P <0.001)。因此,平均速度显著增加(IVC 为 12,Q1-Q3 为 11-14cm/s)与导管为 25,Q1-Q3 为 17-31cm/s,P <0.001),导致中位数 IVC-导管速度不匹配为 1.8(Q1-Q3 为 1.5-2.4),在吸气过程中进一步增加(中位数 2.3,Q1-Q3 为 1.8-3.0)。IVC-导管不匹配与测量的导管尺寸呈负相关,与导管流量呈正相关。呼气和整个呼吸周期的归一化 IVC-导管速度不匹配因子与峰值 VO2 相关(r =-0.37,P =0.014 和 r =-0.31,P =0.04)。
在青少年 Fontan 患者中,从 IVC 到导管观察到重要的血流加速,这与峰值 VO2 有关。因此,本研究引起了人们对植入的 16-20mm 导管对于年龄较大的 Fontan 患者已经变小的担忧,未来的研究应阐明其对长期结果的影响。