Department of Thoracic and Cardiovascular Surgery, International St. Mary's Hospital, Catholic Kwandong University, College of Medicine, Incheon, Korea.
Department of Thoracic and Cardiovascular Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
J Korean Med Sci. 2021 Nov 8;36(43):e266. doi: 10.3346/jkms.2021.36.e266.
This retrospective study investigated the natural course of synchronous ground-glass nodules (GGNs) that remained after curative resection for non-small-cell lung cancer (NSCLC).
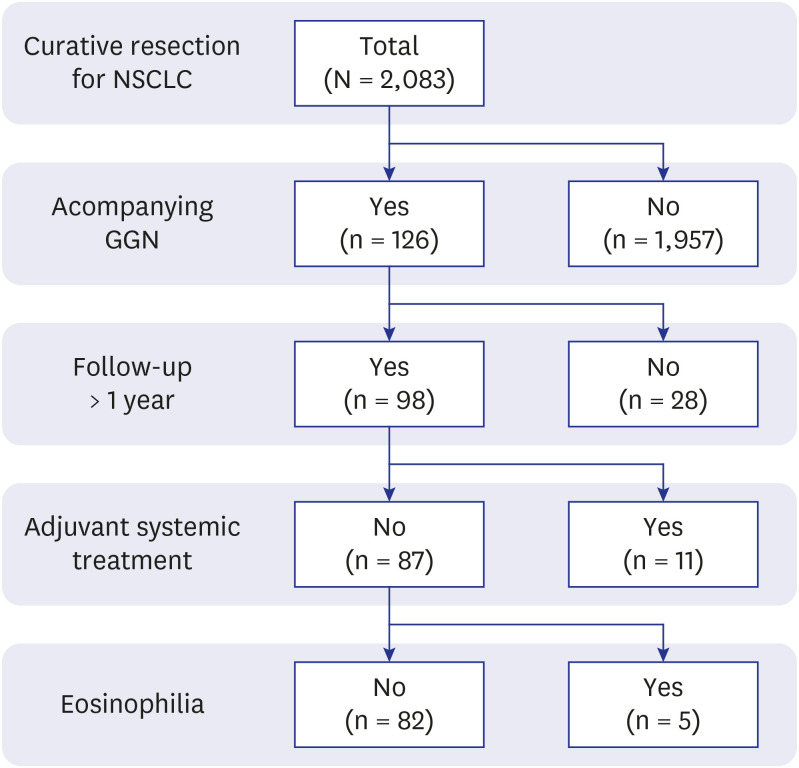
Prospectively collected retrospective data were reviewed concerning 2,276 patients who underwent curative resection for NSCLC between 2008 and 2017. High-resolution computed tomography or thin-section computed tomography data of 82 patients were included in the study. Growth in size was considered the most valuable outcome, and patients were grouped according to GGN size change. Patient demographic data (e.g., age, sex, and smoking history), perioperative data (e.g., GGN characteristics, histopathology and pathological stage of the resected tumours), and other medical history were evaluated in a risk factor analysis concerning GGN size change.
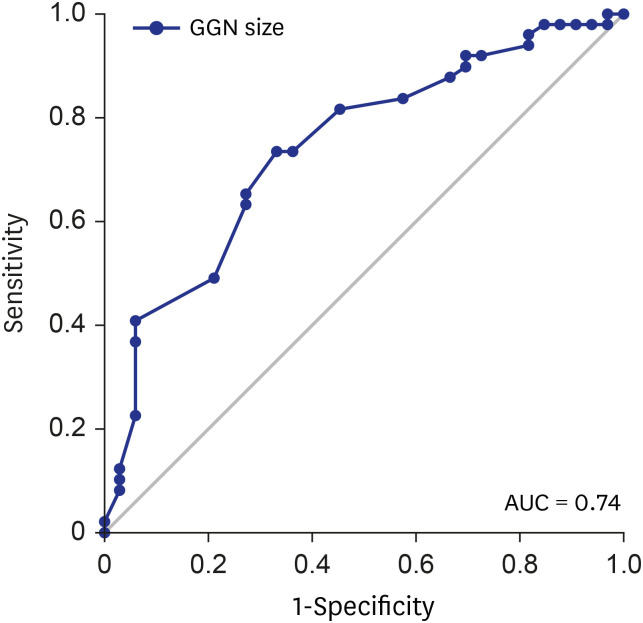
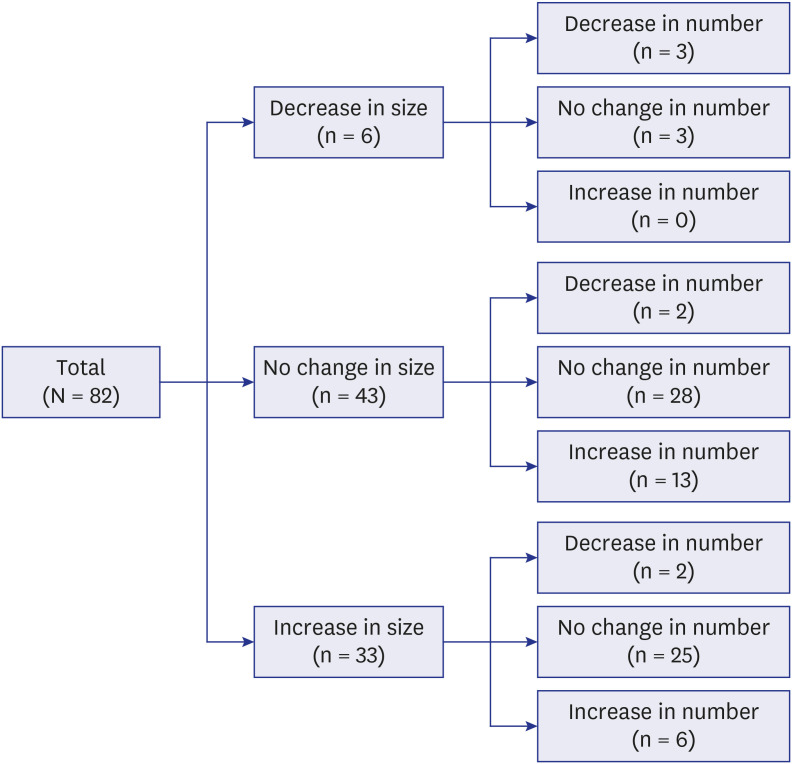
The median duration of follow-up was 36.0 months (interquartile range, 23.0-59.3 months). GGN size decreased in 6 patients (7.3%), was stationary in 43 patients (52.4%), and increased in 33 patients (40.2%). In univariate analysis, male sex, the GGN size on initial CT, part-solid GGN and smoking history (≥ 10 pack-years) were significant risk factors. Among them, multivariate analysis revealed that lager GGN size, part-solid GGN and smoking history were independent risk factors.
During follow-up, 40.2% of GGNs increased in size, emphasising that patients with larger GGNs, part-solid GGN or with a smoking history should be observed.
本回顾性研究调查了非小细胞肺癌(NSCLC)根治性切除术后持续存在的同步磨玻璃结节(GGN)的自然病程。
回顾性分析了 2008 年至 2017 年间接受 NSCLC 根治性切除术的 2276 例患者的前瞻性收集的回顾性数据。研究纳入了 82 例患者的高分辨率 CT 或薄层 CT 数据。大小的增长被认为是最有价值的结果,根据 GGN 大小的变化将患者分组。在 GGN 大小变化的危险因素分析中,评估了患者的人口统计学数据(如年龄、性别和吸烟史)、围手术期数据(如 GGN 特征、切除肿瘤的组织病理学和病理分期)和其他病史。
中位随访时间为 36.0 个月(四分位距 23.0-59.3 个月)。6 例(7.3%)患者的 GGN 大小减小,43 例(52.4%)患者的 GGN 大小不变,33 例(40.2%)患者的 GGN 大小增大。单因素分析显示,男性、初始 CT 上的 GGN 大小、部分实性 GGN 和吸烟史(≥10 包年)是显著的危险因素。其中,多因素分析显示,较大的 GGN 大小、部分实性 GGN 和吸烟史是独立的危险因素。
在随访期间,40.2%的 GGN 大小增加,这强调了对于 GGN 较大、部分实性 GGN 或有吸烟史的患者应进行观察。