University of Chicago, Chicago, Illinois.
Ultromics, Oxford, United Kingdom.
J Am Soc Echocardiogr. 2022 Mar;35(3):295-304. doi: 10.1016/j.echo.2021.10.015. Epub 2021 Nov 6.
COVID-19 infection is known to cause a wide array of clinical chronic sequelae, but little is known regarding the long-term cardiac complications. We aim to report echocardiographic follow-up findings and describe the changes in left (LV) and right ventricular (RV) function that occur following acute infection.
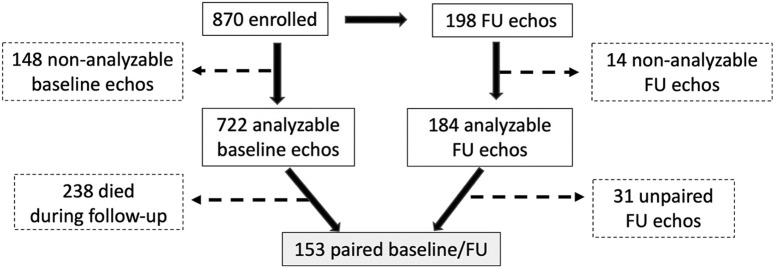
Patients enrolled in the World Alliance Societies of Echocardiography-COVID study with acute COVID-19 infection were asked to return for a follow-up transthoracic echocardiogram. Overall, 198 returned at a mean of 129 days of follow-up, of which 153 had paired baseline and follow-up images that were analyzable, including LV volumes, ejection fraction (LVEF), and longitudinal strain (LVLS). Right-sided echocardiographic parameters included RV global longitudinal strain, RV free wall strain, and RV basal diameter. Paired echocardiographic parameters at baseline and follow-up were compared for the entire cohort and for subgroups based on the baseline LV and RV function.
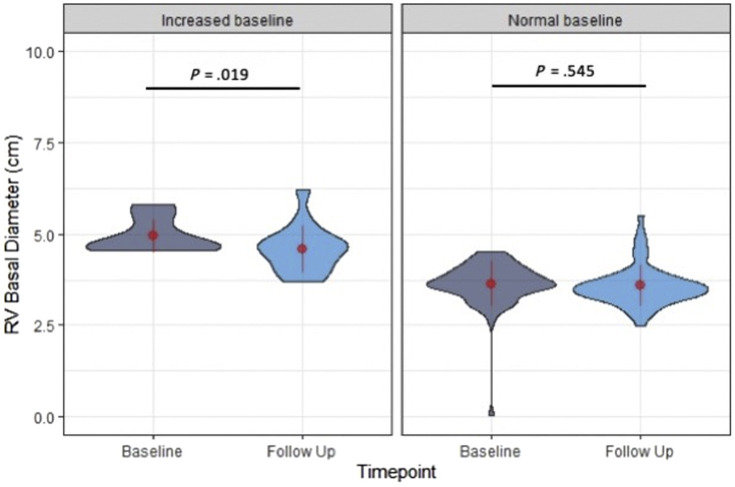
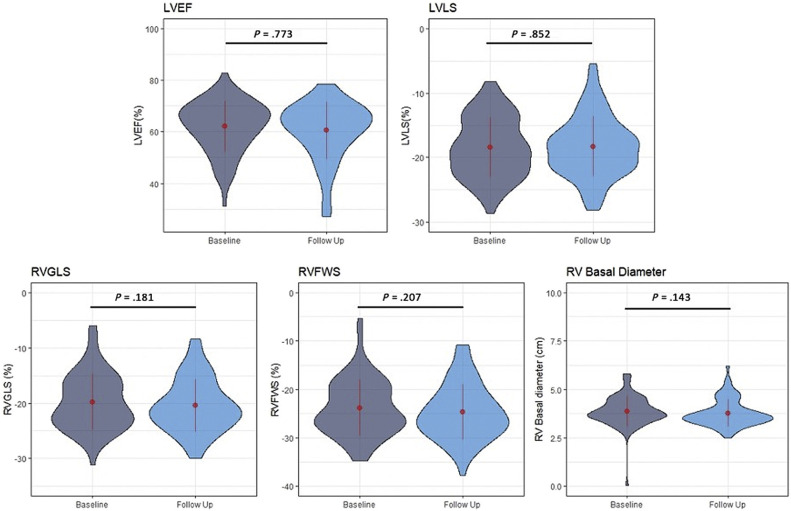
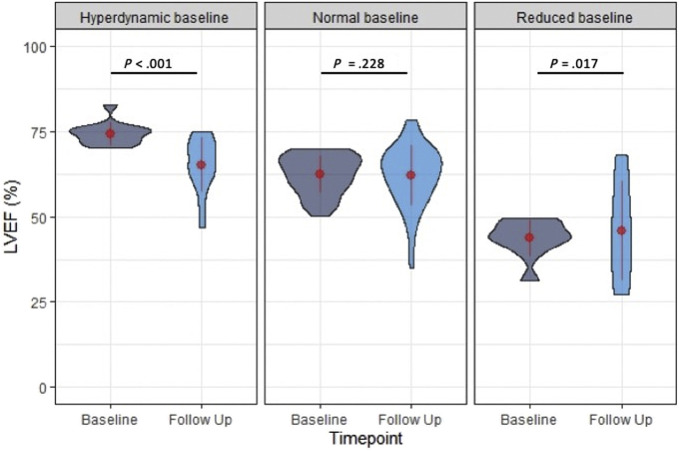
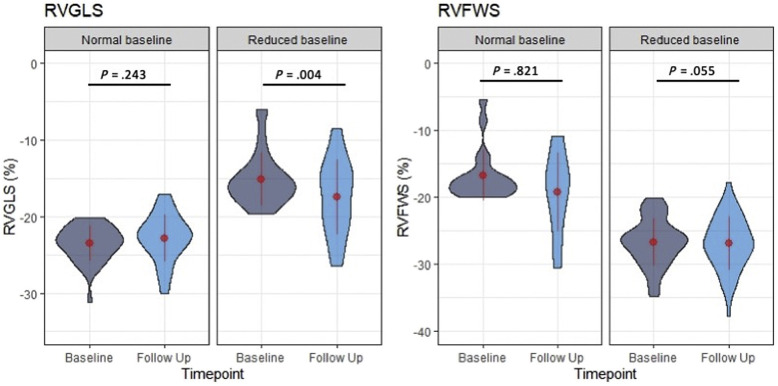
For the entire cohort, echocardiographic markers of LV and RV function at follow-up were not significantly different from baseline (all P > .05). Patients with hyperdynamic LVEF at baseline (>70%), had a significant reduction of LVEF at follow-up (74.3% ± 3.1% vs 64.4% ± 8.1%, P < .001), while patients with reduced LVEF at baseline (<50%) had a significant increase (42.5% ± 5.9% vs 49.3% ± 13.4%, P = .02), and those with normal LVEF had no change. Patients with normal LVLS (<-18%) at baseline had a significant reduction of LVLS at follow-up (-21.6% ± 2.6% vs -20.3% ± 4.0%, P = .006), while patients with impaired LVLS at baseline had a significant improvement at follow-up (-14.5% ± 2.9% vs -16.7% ± 5.2%, P < .001). Patients with abnormal RV global longitudinal strain (>-20%) at baseline had significant improvement at follow-up (-15.2% ± 3.4% vs -17.4% ± 4.9%, P = .004). Patients with abnormal RV basal diameter (>4.5 cm) at baseline had significant improvement at follow-up (4.9 ± 0.7 cm vs 4.6 ± 0.6 cm, P = .019).
Overall, there were no significant changes over time in the LV and RV function of patients recovering from COVID-19 infection. However, differences were observed according to baseline LV and RV function, which may reflect recovery from the acute myocardial injury occurring in the acutely ill. Left ventricular and RV function tends to improve in those with impaired baseline function, while it tends to decrease in those with hyperdynamic LV or normal RV function.
已知 COVID-19 感染可引起广泛的临床慢性后遗症,但对长期心脏并发症知之甚少。我们旨在报告超声心动图随访结果,并描述急性感染后左(LV)和右心室(RV)功能的变化。
在世界超声心动图学会联盟 COVID 研究中招募了患有急性 COVID-19 感染的患者,并要求他们返回进行随访经胸超声心动图检查。共有 198 名患者在平均 129 天的随访中返回,其中 153 名患者具有基线和随访的配对图像,可进行分析,包括 LV 容积、射血分数(LVEF)和纵向应变(LVLS)。右侧超声心动图参数包括 RV 整体纵向应变、RV 游离壁应变和 RV 基底直径。比较整个队列和基于基线 LV 和 RV 功能的亚组的基线和随访时的配对超声心动图参数。
对于整个队列,LV 和 RV 功能的超声心动图标志物在随访时与基线相比没有显著差异(均 P >.05)。基线时射血分数高(>70%)的患者,随访时射血分数明显降低(74.3%±3.1% vs 64.4%±8.1%,P<.001),而基线时射血分数降低(<50%)的患者射血分数显著增加(42.5%±5.9% vs 49.3%±13.4%,P=.02),而射血分数正常的患者没有变化。基线时 LVLS 正常(<-18%)的患者,随访时 LVLS 明显下降(-21.6%±2.6% vs -20.3%±4.0%,P=.006),而基线时 LVLS 受损的患者随访时明显改善(-14.5%±2.9% vs -16.7%±5.2%,P<.001)。基线时 RV 整体纵向应变异常(>-20%)的患者,随访时明显改善(-15.2%±3.4% vs -17.4%±4.9%,P=.004)。基线时 RV 基底直径异常(>4.5 cm)的患者,随访时明显改善(4.9±0.7 cm vs 4.6±0.6 cm,P=.019)。
总体而言,从 COVID-19 感染中恢复的患者的 LV 和 RV 功能在随访期间没有明显变化。然而,根据基线 LV 和 RV 功能观察到差异,这可能反映了急性疾病中发生的急性心肌损伤的恢复。基线功能受损的患者的左心室和 RV 功能趋于改善,而 LV 射血分数高或 RV 功能正常的患者的左心室和 RV 功能趋于下降。