Division of Esophageal Surgery, Akita University Hospital, Akita, Japan.
Department of Thoracic Surgery, Akita University Graduate School of Medicine, Akita, Japan.
BMC Cancer. 2021 Nov 9;21(1):1192. doi: 10.1186/s12885-021-08918-x.
Tumor regression grade (TRG) after neoadjuvant therapy is reportedly predictive of prognosis in esophageal cancer patients, as lack of a response to neoadjuvant therapy is associated with a poor prognosis. However, there is little information available on the timing and pattern of recurrence after esophagectomy for thoracic esophageal squamous cell carcinoma (TESCC) that takes into consideration TRG after neoadjuvant chemoradiotherapy (NACRT). Here, in an effort to gain insight into a treatment strategy that improves the prognosis of NACRT non-responders, we evaluated the patterns and timing of recurrence in TESCC patients, taking into consideration TRG after NACRT.
A total of 127 TESCC patients treated with NACRT and esophagectomy between 2009 and 2017 were enrolled in this observational cohort study. TRGs were assigned based on the proportion of residual tumor cells in the area (TRG1, ≥1/3 viable cancer cells; 2, < 1/3 viable cancer cells; 3, no viable cancer cells). We retrospectively investigated the timing and patterns of recurrence and the prognoses in TESCC patients, taking into consideration TRG after NACRT.
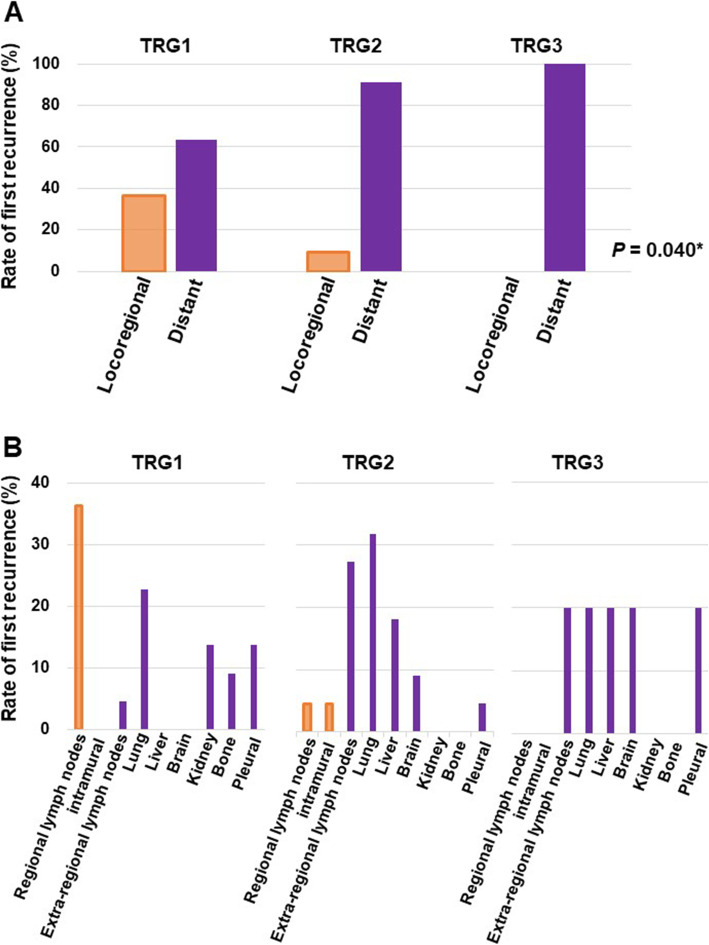
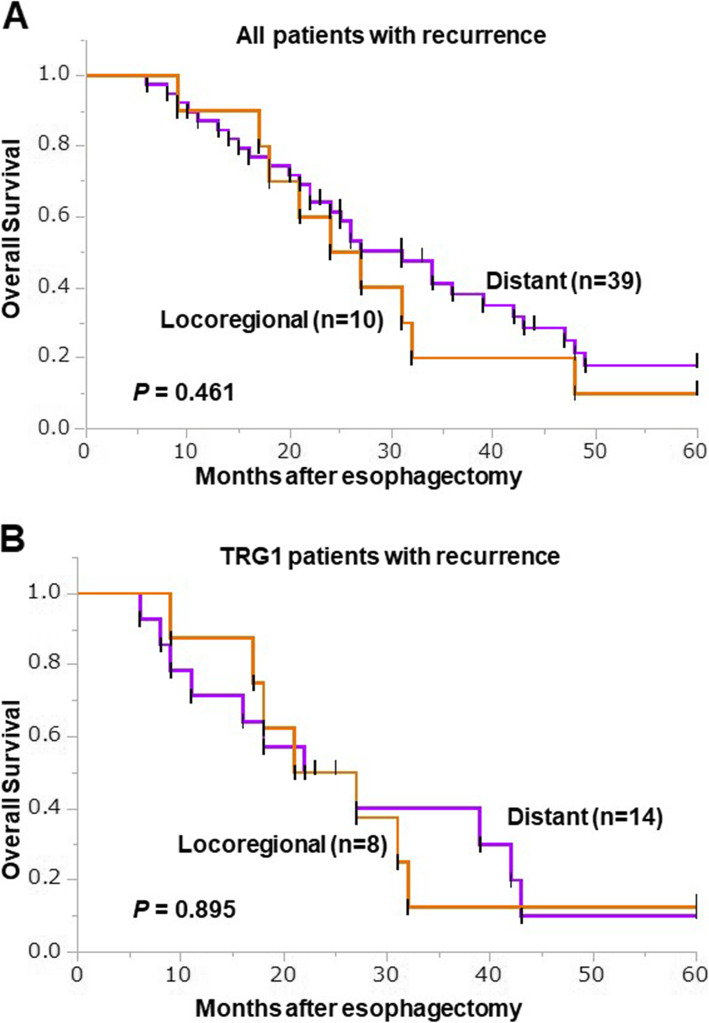
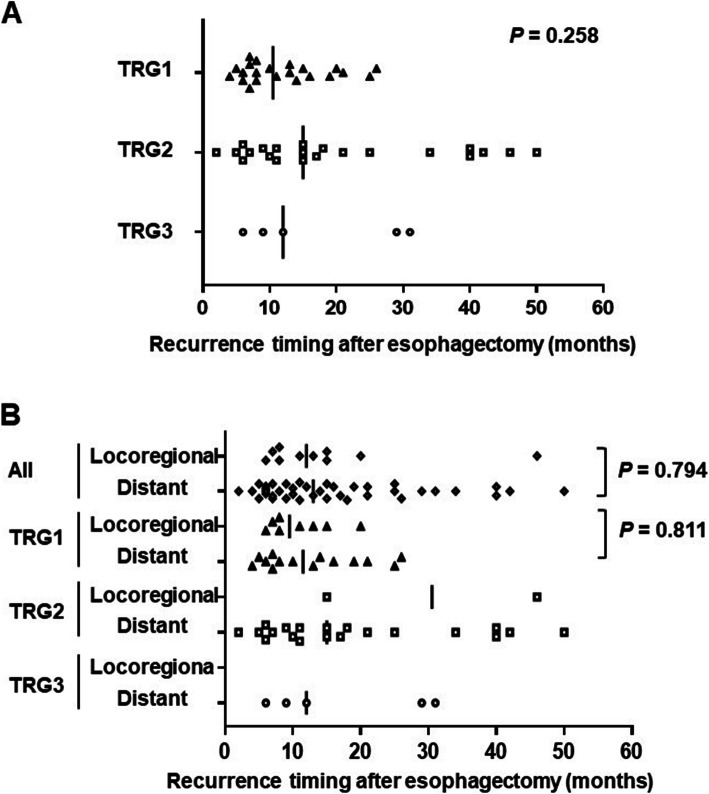
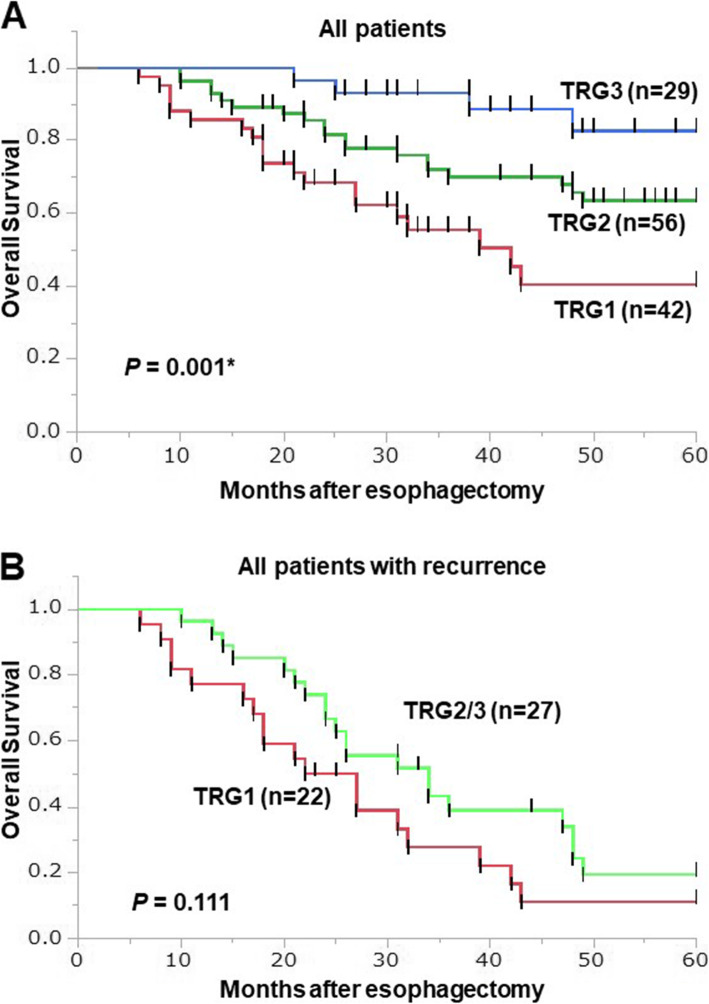
The 127 participating TESCC patients were categorized as TRG1 (42 patients, 33%), TRG2 (56 patients, 44%) or TRG3 (29 patients, 23%). The locoregional recurrence rate was higher in TRG1 (36.4%) patients than combined TRG2-3 (7.4%) patients. Patients with TRG3 had better prognoses, though a few TRG3 patients experienced distant recurrence. There were no significant differences in median time to first recurrence or OS among patients with locoregional or distant recurrence. There was a trend toward better OS in TRG2-3 patients with recurrence than TRG1 patients with recurrence, but the difference was not significant.
NACRT non-responders (TRG1 patients) experienced higher locoregional recurrence rates and earlier recurrence with distant or locoregional metastasis. TRG appears to be useful for establishing a strategy for perioperative treatments to improve TESCC patient survival, especially among TRG1 patients. (303 words).
据报道,新辅助治疗后的肿瘤退缩分级(TRG)可预测食管癌患者的预后,因为对新辅助治疗无反应与预后不良相关。然而,对于接受新辅助放化疗(NACRT)后的胸段食管鳞状细胞癌(TESCC)患者,关于手术后复发的时间和模式,几乎没有考虑到新辅助放化疗后 TRG 的相关信息。在这里,为了深入了解改善 NACRT 无反应者预后的治疗策略,我们评估了考虑到 NACRT 后 TRG 的 TESCC 患者的复发模式和时间。
本观察性队列研究共纳入 2009 年至 2017 年间接受 NACRT 和食管切除术治疗的 127 例 TESCC 患者。根据残留肿瘤细胞比例(TRG1,≥1/3 活癌细胞;2,<1/3 活癌细胞;3,无活癌细胞)分配 TRG。我们回顾性研究了 TESCC 患者在考虑到 NACRT 后 TRG 的情况下,复发的时间和模式以及预后。
127 例参与的 TESCC 患者被分为 TRG1(42 例,33%)、TRG2(56 例,44%)或 TRG3(29 例,23%)。TRG1(36.4%)患者的局部区域复发率高于联合 TRG2-3(7.4%)患者。TRG3 患者的预后较好,但少数 TRG3 患者出现远处复发。局部或远处复发患者的首次复发中位时间或 OS 无显著差异。有远处复发的 TRG2-3 患者的 OS 有改善趋势,但差异无统计学意义。
NACRT 无反应者(TRG1 患者)出现较高的局部区域复发率,较早出现远处转移或局部区域转移的复发。TRG 似乎可用于制定围手术期治疗策略,以改善 TESCC 患者的生存,尤其是 TRG1 患者。(303 字)