Yunusa Ismaeel, Alsahali Saud, Rane Amey, Eguale Tewodros
Center for Outcomes Research and Evaluation, Department of Clinical Pharmacy and Outcomes Sciences, University of South Carolina College of Pharmacy, Columbia, SC, USA.
Department of Pharmacy Practice, Unaizah College of Pharmacy, Qassim University, Qassim, Saudi Arabia.
J Alzheimers Dis Rep. 2021 Sep 6;5(1):705-713. doi: 10.3233/ADR-210307. eCollection 2021.
Pharmacological treatment of Alzheimer's disease (AD) involves symptomatic improvement of cognition using cholinesterase inhibitors (ChEIs) and memantine. The cost-effectiveness of these medications will guide decision-makers in making judicious use of scarce healthcare resources, particularly during the advanced disease stages.
To evaluate the cost-effectiveness of ChEIs, memantine, and ChEI-memantine combinations in persons with moderate-to-severe AD from the US healthcare perspective.
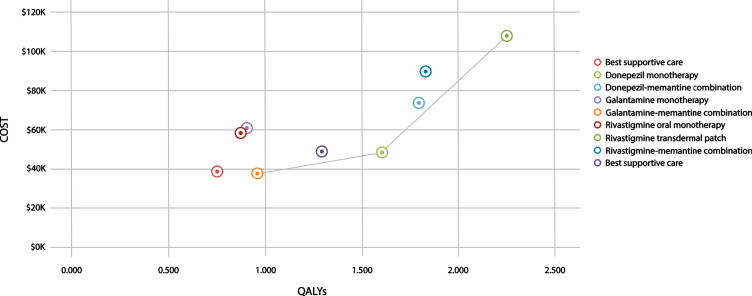
This pharmacoeconomic evaluation study used a state-transition Markov cohort model to simulate the costs and effectiveness of ChEI-memantine combinations compared with monotherapies of ChEI (donepezil, galantamine and rivastigmine) and memantine in persons with moderate-to-severe AD over a lifetime horizon with a 1-year cycle length. We estimated expected quality-adjusted life-years (QALYs), costs (in 2020 $US), net monetary benefits, and incremental cost-effectiveness ratios (ICERs). We discounted future costs and QALYs at the rate of 3%.
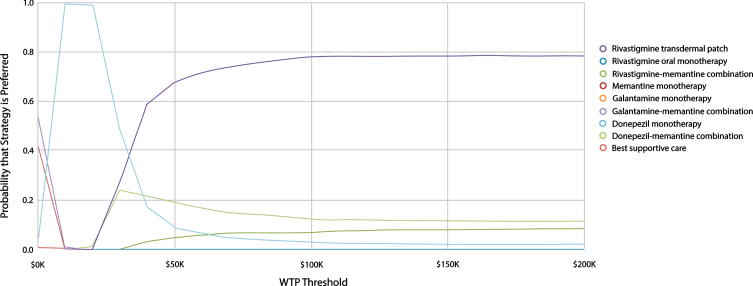
In this study, donepezil monotherapy, galantamine-memantine combination, and rivastigmine transdermal patch formed the cost-effectiveness frontier. Findings suggests that rivastigmine transdermal patch is the optimal treatment strategy at a willingness-to-pay (WTP) threshold of $150,000/QALY (ICER = $93,307/QALY [versus donepezil monotherapy]). Results across subgroups by age and sex also suggest that the rivastigmine transdermal patch is the optimal treatment strategy with the highest net benefit.
From the US healthcare perspective, we found that, for persons with moderate-to-severe AD at a WTP threshold of $150,000/QALY, the rivastigmine transdermal patch is the most cost-effective pharmacological treatment option. Given that the transdermal patch is a preferred route of administration for persons with AD and their caregivers due to its convenience, our findings provide additional incentives for its use.
阿尔茨海默病(AD)的药物治疗包括使用胆碱酯酶抑制剂(ChEIs)和美金刚来改善认知症状。这些药物的成本效益将指导决策者合理使用稀缺的医疗资源,尤其是在疾病晚期。
从美国医疗保健的角度评估ChEIs、美金刚以及ChEI-美金刚联合用药在中重度AD患者中的成本效益。
这项药物经济学评估研究使用了一种状态转换马尔可夫队列模型,以模拟在整个生命周期且周期长度为1年的情况下,ChEI-美金刚联合用药与ChEI(多奈哌齐、加兰他敏和卡巴拉汀)及美金刚单药治疗相比的成本和效果。我们估计了预期的质量调整生命年(QALYs)、成本(以2020年美元计)、净货币效益和增量成本效益比(ICERs)。我们以3%的贴现率对未来成本和QALYs进行贴现。
在本研究中,多奈哌齐单药治疗、加兰他敏-美金刚联合用药以及卡巴拉汀透皮贴剂构成了成本效益前沿。研究结果表明,在支付意愿(WTP)阈值为150,000美元/QALY时,卡巴拉汀透皮贴剂是最佳治疗策略(ICER = 93,307美元/QALY [相对于多奈哌齐单药治疗])。按年龄和性别划分的亚组结果也表明,卡巴拉汀透皮贴剂是净效益最高的最佳治疗策略。
从美国医疗保健的角度来看,我们发现,对于支付意愿阈值为150,000美元/QALY的中重度AD患者,卡巴拉汀透皮贴剂是最具成本效益的药物治疗选择。鉴于透皮贴剂因其便利性而成为AD患者及其护理人员首选的给药途径,我们的研究结果为其使用提供了更多激励。