Kuo Yuan-Hung, Lu Sheng-Nan, Chen Yen-Yang, Kee Kwong-Ming, Yen Yi-Hao, Hung Chao-Hung, Hu Tsung-Hui, Chen Chien-Hung, Wang Jing-Houng
Division of Hepatogastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan.
Division of Hematology-Oncology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan.
Front Oncol. 2021 Oct 25;11:737767. doi: 10.3389/fonc.2021.737767. eCollection 2021.
Lenvatinib is approved for patients with advanced hepatocellular carcinoma (HCC) due to its non-inferiority to sorafenib of overall survival (OR) in clinical trials. This study was to compare the effectiveness and safety of lenvatinib and sorafenib in the real world.
We retrospectively evaluated 338 patients with unresectable HCC who had undergone lenvatinib or sorafenib treatment between January 2018 and August 2020. Propensity-score matching analysis was performed with a 1:2 ratio to reduce the real-life baseline difference between the two groups.
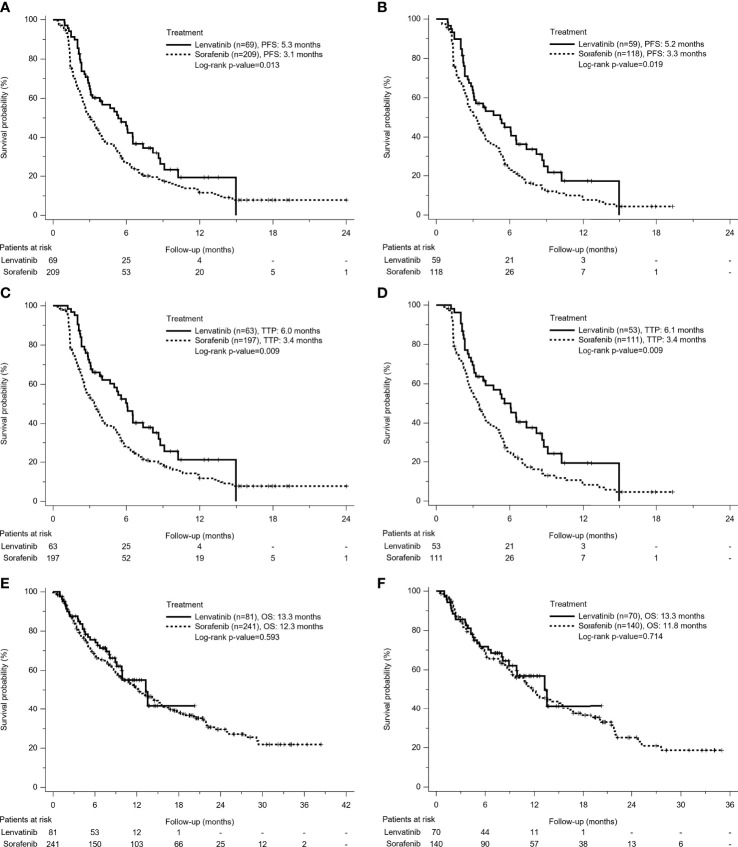
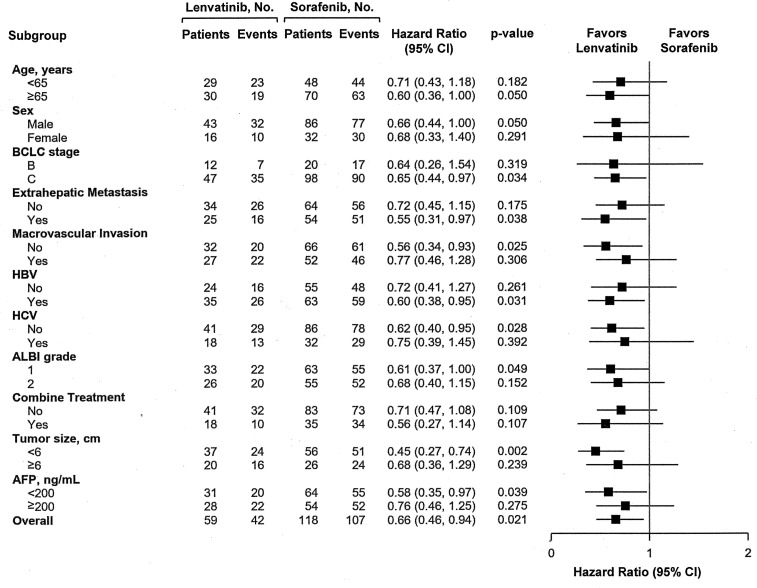
A total of 210 patients (Male/Female: 150/60, mean age: 65.8 years) were recruited including 70 patients in the Lenvatinib group and 140 patients in the Sorafenib group. Compared with sorafenib, lenvatinib had significantly longer progression-free survival (PFS) (5.2 3.3 months, p=0.019) but similar OR (13.3 11.8 months, p=0.714). Additionally, lenvatinib had better disease control rates (62.3 48.6%, p=0.029) and equivalent incidences of treatment-related adverse events over sorafenib. In multivariate analysis, lenvatinib was associated with better PFS over sorafenib (hazard ratio: 0.49, 95% confidence interval: 0.3-0.79, p=0.004) after adjustments of albumin-bilirubin grade and alpha-fetoprotein level; however, different agents using lenvatinib or sorafenib did not contribute to OS, whether in univariate or multivariate analysis. Patients who failed lenvatinib had a lower proportion of having sequential systemic therapies compared with the Sorafenib group (36.2 47.8%, p=0.02). The most frequently used sequential therapy following lenvatinib and sorafenib was chemotherapy (n=9, 42.8%) and regorafenib (n=33, 50.8%), respectively.
In clinical real-life practice, lenvatinib illustrated promising survival benefits and acceptable safety for patients with unresectable HCC, while reducing the risk of progression disease compared with sorafenib. Additionally, lack of approved post-lenvatinib systemic therapies is a serious issue in the real world.
由于在临床试验中乐伐替尼的总生存期(OS)不劣于索拉非尼,因此被批准用于晚期肝细胞癌(HCC)患者。本研究旨在比较乐伐替尼和索拉非尼在现实世界中的有效性和安全性。
我们回顾性评估了2018年1月至2020年8月期间接受乐伐替尼或索拉非尼治疗的338例不可切除HCC患者。采用1:2的倾向评分匹配分析以减少两组之间现实生活中的基线差异。
共纳入210例患者(男/女:150/60,平均年龄:65.8岁),其中乐伐替尼组70例,索拉非尼组140例。与索拉非尼相比,乐伐替尼的无进展生存期(PFS)显著更长(5.2对3.3个月,p=0.019),但OS相似(13.3对11.8个月,p=0.714)。此外,乐伐替尼的疾病控制率更高(62.3%对48.6%,p=0.029),且与索拉非尼相比,治疗相关不良事件的发生率相当。在多变量分析中,调整白蛋白-胆红素分级和甲胎蛋白水平后,乐伐替尼与索拉非尼相比PFS更好(风险比:0.49,95%置信区间:0.3-0.79,p=0.004);然而,无论是单变量还是多变量分析,使用乐伐替尼或索拉非尼不同药物对OS均无影响。与索拉非尼组相比,乐伐替尼治疗失败的患者接受序贯全身治疗的比例更低(36.2%对47.8%,p=0.02)。乐伐替尼和索拉非尼之后最常用的序贯治疗分别是化疗(n=9,42.8%)和瑞戈非尼(n=33,50.8%)。
在临床实际应用中,乐伐替尼对不可切除HCC患者显示出有前景的生存获益和可接受的安全性,同时与索拉非尼相比降低了疾病进展风险。此外,现实世界中缺乏获批的乐伐替尼后全身治疗方案是一个严重问题。