Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, 99 Commercial Road, Melbourne, Victoria, 3004, Australia.
Department of Cardiology, University Heart & Vascular Centre, Hamburg, Germany.
Geroscience. 2022 Feb;44(1):403-413. doi: 10.1007/s11357-021-00486-z. Epub 2021 Nov 11.
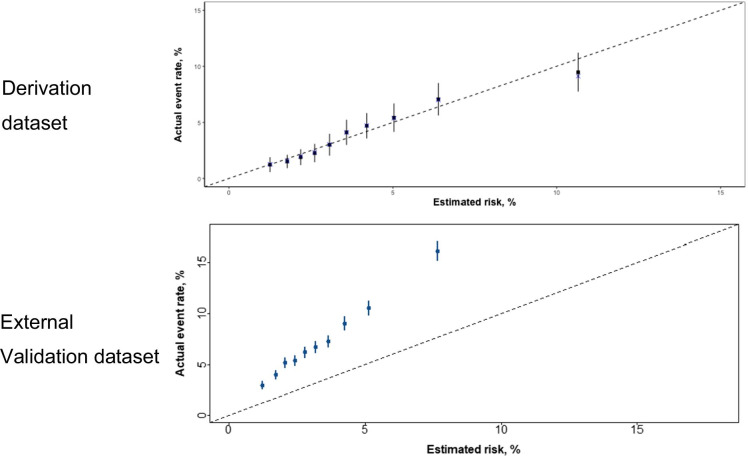
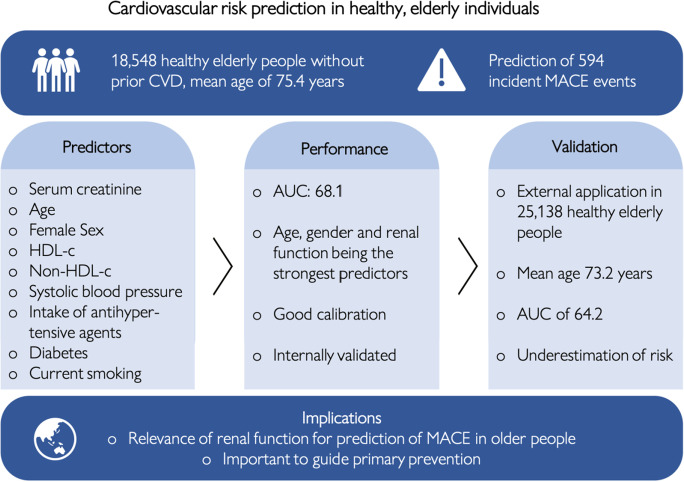
Identification of individuals with increased risk of major adverse cardiovascular events (MACE) is important. However, algorithms specific to the elderly are lacking. Data were analysed from a randomised trial involving 18,548 participants ≥ 70 years old (mean age 75.4 years), without prior cardiovascular disease events, dementia or physical disability. MACE included coronary heart disease death, fatal or nonfatal ischaemic stroke or myocardial infarction. Potential predictors tested were based on prior evidence and using a machine-learning approach. Cox regression analyses were used to calculate 5-year predicted risk, and discrimination evaluated from receiver operating characteristic curves. Calibration was also assessed, and the findings internally validated using bootstrapping. External validation was performed in 25,138 healthy, elderly individuals in the primary care environment. During median follow-up of 4.7 years, 594 MACE occurred. Predictors in the final model included age, sex, smoking, systolic blood pressure, high-density lipoprotein cholesterol (HDL-c), non-HDL-c, serum creatinine, diabetes and intake of antihypertensive agents. With variable selection based on machine-learning, age, sex and creatinine were the most important predictors. The final model resulted in an area under the curve (AUC) of 68.1 (95% confidence intervals 65.9; 70.4). The model had an AUC of 67.5 in internal and 64.2 in external validation. The model rank-ordered risk well but underestimated absolute risk in the external validation cohort. A model predicting incident MACE in healthy, elderly individuals includes well-recognised, potentially reversible risk factors and notably, renal function. Calibration would be necessary when used in other populations.
识别发生主要不良心血管事件(MACE)风险增加的个体很重要。然而,目前缺乏针对老年人的专门算法。本研究的数据来自一项纳入 18548 名年龄≥70 岁(平均年龄 75.4 岁)、无心血管疾病史、痴呆或身体残疾的参与者的随机试验。MACE 包括冠心病死亡、致死性或非致死性缺血性卒中和心肌梗死。所测试的潜在预测因素基于先前的证据,并采用机器学习方法。使用 Cox 回归分析计算 5 年预测风险,并通过接受者操作特征曲线评估区分度。还评估了校准情况,并使用自举法对内部分值进行验证。外部验证在初级保健环境中 25138 名健康的老年人中进行。中位随访 4.7 年后,发生了 594 例 MACE。最终模型中的预测因素包括年龄、性别、吸烟、收缩压、高密度脂蛋白胆固醇(HDL-c)、非高密度脂蛋白胆固醇(non-HDL-c)、血清肌酐、糖尿病和降压药的使用。基于机器学习的变量选择,年龄、性别和肌酐是最重要的预测因素。最终模型的曲线下面积(AUC)为 68.1(95%置信区间 65.9;70.4)。内部验证的 AUC 为 67.5,外部验证的 AUC 为 64.2。该模型很好地对风险进行了排序,但在外部验证队列中低估了绝对风险。该模型预测健康老年人发生 MACE 的风险包含了公认的、潜在可逆转的风险因素,特别是肾功能。在其他人群中使用时需要进行校准。