Ali Samina, Morrison Ellen, Shwetz Seyara, Yaskina Maryna, Rajagopal Manasi, Estey Andrea, Drendel Amy L
Department of Pediatrics, University of Alberta, Edmonton, Alberta, Canada.
Women and Children's Health Research Institute, Edmonton, Alberta, Canada.
Paediatr Child Health. 2021 May 26;26(7):421-427. doi: 10.1093/pch/pxab011. eCollection 2021 Nov.
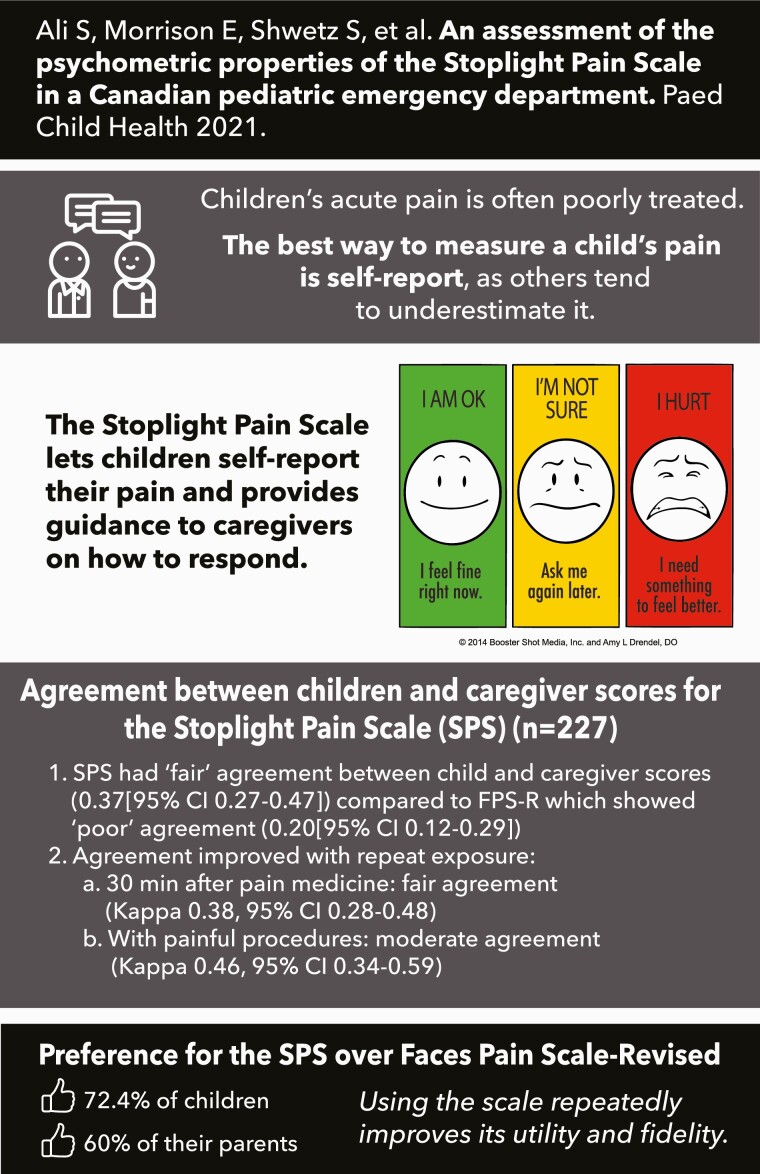
This study aimed to validate a novel, three faced, colour-coded, action-oriented tool: The Stoplight Pain Scale (SPS).
A prospective observational cohort study was conducted at a Canadian paediatric emergency department from November 2014 to February 2017. Patients aged 3 to 12 years and their caregivers were asked to rate pain using the SPS and the Faces Pain Scale-Revised (FPS-R). Pain was measured just before analgesia administration, 30 minutes after analgesia administration, and immediately following a painful procedure.
A total of 227 patients were included; 26.9% (61/227) were 3 to 5 years old while 73.1% (166/227) were 6 to 12 years old. Using Cohen's κ, agreement for SPS and FPS-R was 'fair' for children (0.28 [95% confidence interval {CI} 0.20 to 0.36]) and 'poor' for caregivers (0.14 [95% CI 0.07 to 0.21]), at initial measurement. The SPS had 'fair' agreement between child and caregiver scores, (0.37 [95% CI 0.27 to 0.47]), compared to FPS-R which showed 'poor' agreement (0.20 [95% CI 0.12 to 0.29]). Absolute agreement between child and caregiver SPS scores improved with repeat exposure; 30 minutes after analgesia administration, caregivers and children had fair agreement (κ=0.38, 95% CI 0.28 to 0.48); they had moderate agreement directly following painful procedures (κ=0.46, 95% CI 0.34 to 0.59). Overall, 72.4% (139/192) of children and 60.2% (118/196) of caregivers preferred SPS over FPS-R.
The SPS demonstrates fair agreement with FPS-R for children and fair-moderate agreement between children and caregivers; agreement improved with repeat use. The SPS is simple and easy to use; it may have a role in empowering direct child and family involvement in pain management.
本研究旨在验证一种新型的、三面的、颜色编码的、以行动为导向的工具:红绿灯疼痛量表(SPS)。
2014年11月至2017年2月在加拿大一家儿科急诊科进行了一项前瞻性观察队列研究。邀请3至12岁的患者及其护理人员使用SPS和面部疼痛量表修订版(FPS-R)对疼痛进行评分。在给予镇痛药物之前、给予镇痛药物30分钟后以及在进行疼痛操作后立即测量疼痛。
共纳入227例患者;26.9%(61/227)为3至5岁,73.1%(166/227)为6至12岁。使用科恩κ系数,在初始测量时,儿童中SPS与FPS-R的一致性为“一般”(0.28[95%置信区间{CI}0.20至0.36]),护理人员中为“较差”(0.14[95%CI0.07至0.21])。与FPS-R显示“较差”一致性(0.20[95%CI0.12至0.29])相比,SPS在儿童和护理人员评分之间具有“一般”一致性(0.37[95%CI0.27至0.47])。随着重复使用,儿童和护理人员SPS评分之间的绝对一致性有所提高;给予镇痛药物30分钟后,护理人员和儿童具有一般一致性(κ=0.38,95%CI0.28至0.48);在疼痛操作后立即具有中等一致性(κ=0.46,95%CI0.34至0.59)。总体而言,72.4%(139/192)的儿童和60.2%(118/196)的护理人员更喜欢SPS而不是FPS-R。
SPS在儿童中与FPS-R显示出一般一致性,在儿童和护理人员之间显示出一般至中等一致性;随着重复使用,一致性有所提高。SPS简单易用;它可能在使儿童和家庭直接参与疼痛管理方面发挥作用。