Lemoine Pauline, Bruand Marie, Kammerer Emmanuel, Bogart Emilie, Comte Pauline, Royer Philippe, Thariat Juliette, Pasquier David
Academic Department of Radiation Oncology, O. Lambret Center, Lille, France.
University of Lille, H. Warembourg School of Medicine, Lille, France.
Front Oncol. 2021 Oct 28;11:736690. doi: 10.3389/fonc.2021.736690. eCollection 2021.
Stereotactic radiotherapy may improve the prognosis of oligometastatic patients. In the literature, there is very little data available that is specific to breast cancer.
We conducted a multicenter retrospective study. The primary objective was to estimate progression-free survival after stereotactic body radiotherapy (SBRT) using Cyberknife of breast cancer oligometastases. The secondary objectives were to estimate overall survival, local control, and toxicity. The inclusion criteria were oligometastatic breast cancer with a maximum of five lesions distributed in one to three different organs, diagnosed on PET/CT and/or MRI, excluding brain metastases and oligoprogressions. This was combined with systemic medical treatment.
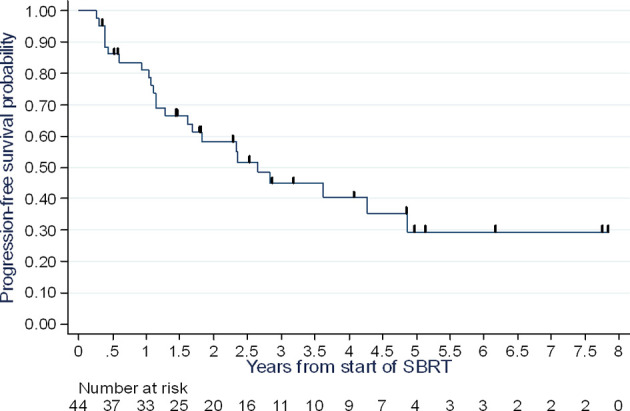
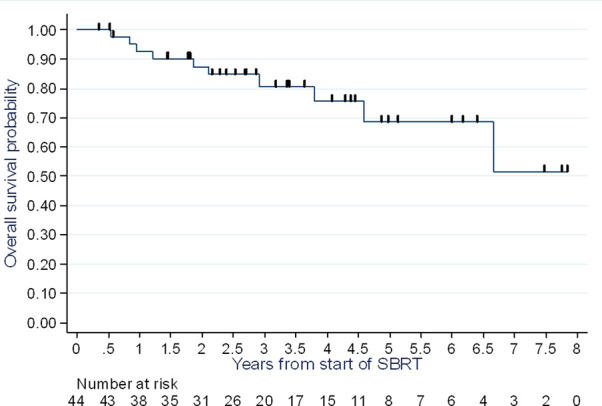
Forty-four patients were enrolled from 2007 to 2017, at three high-volume cancer centers. The patients mostly had one to two lesion(s) whose most widely represented site was bone (24 lesions or 44.4%), particularly in the spine, followed by liver (22 lesions or 40.7%), then pulmonary lesions (six lesions or 11.1%). The primary tumor expressed estrogen receptors in 33 patients (84.6%); the status was HER2+++ in 7 patients (17.9%). The median dose was 40 Gy (min-max: 15-54) prescribed at 80% isodose, the median number of sessions was three (min-max: 3-10). The median D50% was 42 Gy (min max 17-59). After a median follow-up of 3.4 years, progression-free survival (PFS) at one year, two years, and three years was 81% (95% CI: 66-90%), 58% (95% CI: 41-72%), and 45% (95% CI: 28-60%), respectively. The median PFS was 2.6 years (95% CI: 1.3 - 4.9). Overall survival at three years was 81% (95% CI: 63-90%). The local control rate at two and three years was 100%. Three patients (7.3%) experienced G2 acute toxicity, no grade ≥3 toxicity was reported.
The PFS of oligometastatic breast cancer patients treated with SBRT appears long, with low toxicity. Local control is high. SBRT for oligometastases is rarely applied in breast cancer in light of the population in our study. Phase III studies are ongoing.
立体定向放射治疗可能改善寡转移患者的预后。在文献中,很少有针对乳腺癌的具体数据。
我们进行了一项多中心回顾性研究。主要目的是评估使用射波刀对乳腺癌寡转移灶进行立体定向体部放射治疗(SBRT)后的无进展生存期。次要目的是评估总生存期、局部控制率和毒性。纳入标准为寡转移乳腺癌,最多五个病灶分布于一至三个不同器官,通过PET/CT和/或MRI诊断,排除脑转移和寡进展。这与全身药物治疗相结合。
2007年至2017年期间,在三个大型癌症中心共纳入44例患者。患者大多有一至两个病灶,最常见的部位是骨(24个病灶,占44.4%),尤其在脊柱,其次是肝(22个病灶,占40.7%),然后是肺部病灶(6个病灶,占11.1%)。33例患者(84.6%)的原发肿瘤表达雌激素受体;7例患者(17.9%)的状态为HER2+++。中位剂量为40 Gy(最小-最大:15 - 54),按80%等剂量线处方,中位疗程数为3次(最小-最大:3 - 10)。中位D50%为42 Gy(最小-最大:17 - 59)。中位随访3.4年后,1年、2年和3年的无进展生存期(PFS)分别为81%(95%CI:66 - 90%)、58%(95%CI:41 - 72%)和45%(95%CI:28 - 60%)。中位PFS为2.6年(95%CI:1.3 - 4.9)。3年总生存率为81%(95%CI:63 - 90%)。2年和3年的局部控制率为100%。3例患者(7.3%)出现2级急性毒性,未报告≥3级毒性。
接受SBRT治疗的寡转移乳腺癌患者的PFS似乎较长,毒性较低。局部控制率高。鉴于我们研究中的人群,SBRT用于寡转移在乳腺癌中很少应用。III期研究正在进行中。