Sarma Moinak Sen, Seetharaman Jayendra
Department of Pediatric Gastroenterology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow 226014, Uttar Pradesh, India.
World J Hepatol. 2021 Oct 27;13(10):1269-1288. doi: 10.4254/wjh.v13.i10.1269.
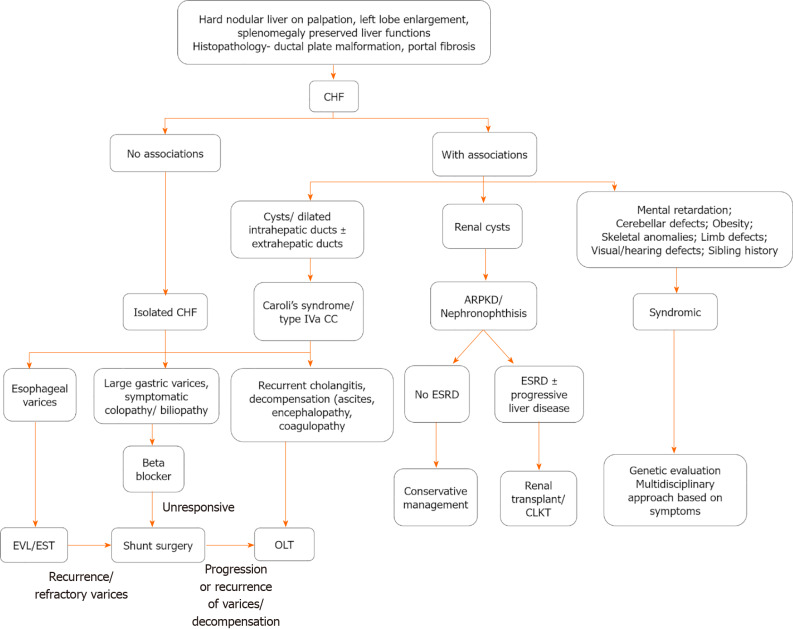
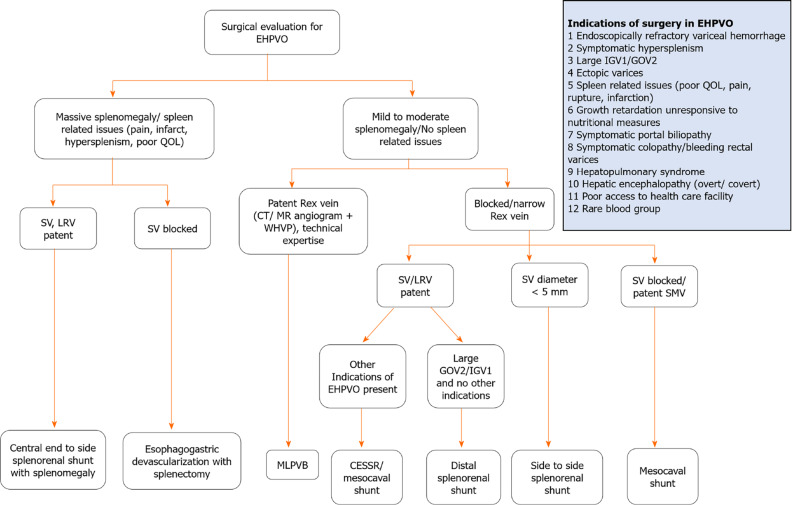
Non-cirrhotic portal hypertension (NCPH) forms an important subset of portal hypertension in children. Variceal bleed and splenomegaly are their predominant presentation. Laboratory features show cytopenias (hypersplenism) and preserved hepatic synthetic functions. Repeated sessions of endoscopic variceal ligation or endoscopic sclerotherapy eradicate esophageal varices in almost all cases. After variceal eradication, there is an increased risk of other complications like secondary gastric varices, cholangiopathy, colopathy, growth failure, especially in extra-hepatic portal vein obstruction (EHPVO). Massive splenomegaly-related pain and early satiety cause poor quality of life (QoL). Meso-Rex bypass is the definitive therapy when the procedure is anatomically feasible in EHPVO. Other portosystemic shunt surgeries with splenectomy are indicated when patients present late and spleen-related issues predominate. Shunt surgeries prevent rebleed, improve growth and QoL. Non-cirrhotic portal fibrosis (NCPF) is a less common cause of portal hypertension in children in developing nations. Presentation in the second decade, massive splenomegaly and patent portal vein are discriminating features of NCPF. Shunt surgery is required in severe cases when endotherapy is insufficient for the varices. Congenital hepatic fibrosis (CHF) presents with firm palpable liver and splenomegaly. Ductal plate malformation forms the histological hallmark of CHF. CHF is commonly associated with Caroli's disease, renal cysts, and syndromes associated with neurological defects. Isolated CHF has a favourable prognosis requiring endotherapy. Liver transplantation is required when there is decompensation or recurrent cholangitis, especially in Caroli's syndrome. Combined liver-kidney transplantation is indicated when both liver and renal issues are present.
非肝硬化性门静脉高压症(NCPH)是儿童门静脉高压症的一个重要亚型。静脉曲张破裂出血和脾肿大是其主要表现。实验室检查特征显示血细胞减少(脾功能亢进)且肝脏合成功能保留。几乎在所有病例中,反复进行内镜下静脉曲张结扎术或内镜硬化治疗可消除食管静脉曲张。静脉曲张消除后,出现其他并发症的风险增加,如继发性胃静脉曲张、胆管病、结肠病、生长发育迟缓,尤其是在肝外门静脉阻塞(EHPVO)时。巨大脾肿大相关的疼痛和早饱会导致生活质量(QoL)下降。当手术在解剖学上可行时,Meso-Rex分流术是EHPVO的确定性治疗方法。当患者就诊较晚且以脾脏相关问题为主时,可进行其他门体分流手术并联合脾切除术。分流手术可预防再出血,改善生长发育和生活质量。在发展中国家,非肝硬化性门静脉纤维化(NCPF)是儿童门静脉高压症较不常见的病因。发病于第二个十年、巨大脾肿大和门静脉通畅是NCPF的鉴别特征。在内科治疗对静脉曲张不足时,严重病例需要进行分流手术。先天性肝纤维化(CHF)表现为肝脏质地变硬可触及和脾肿大。导管板畸形是CHF的组织学特征。CHF通常与卡罗利病、肾囊肿以及与神经缺陷相关的综合征有关。孤立性CHF预后良好,需要内科治疗。当出现失代偿或复发性胆管炎时,尤其是在卡罗利综合征中,需要进行肝移植。当肝脏和肾脏问题均存在时,需要进行肝肾联合移植。