Department of Medical Oncology, Division of Hematologic Malignancies, Dana-Farber Cancer Institute, Boston, MA.
Department of Data Science, Dana Farber Cancer Institute, Boston, MA.
J Clin Oncol. 2022 Jan 10;40(2):189-201. doi: 10.1200/JCO.21.02286. Epub 2021 Nov 18.
Clonal hematopoiesis (CH) can be transmitted from a donor to a recipient during allogeneic hematopoietic cell transplantation. Exclusion of candidate donors with CH is controversial since its impact on recipient outcomes and graft alloimmune function is uncertain.
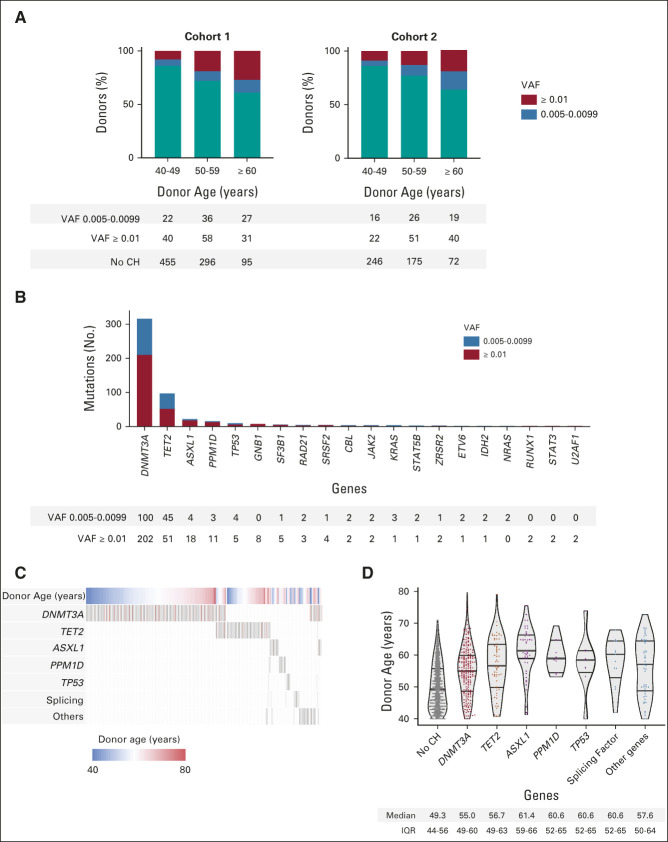
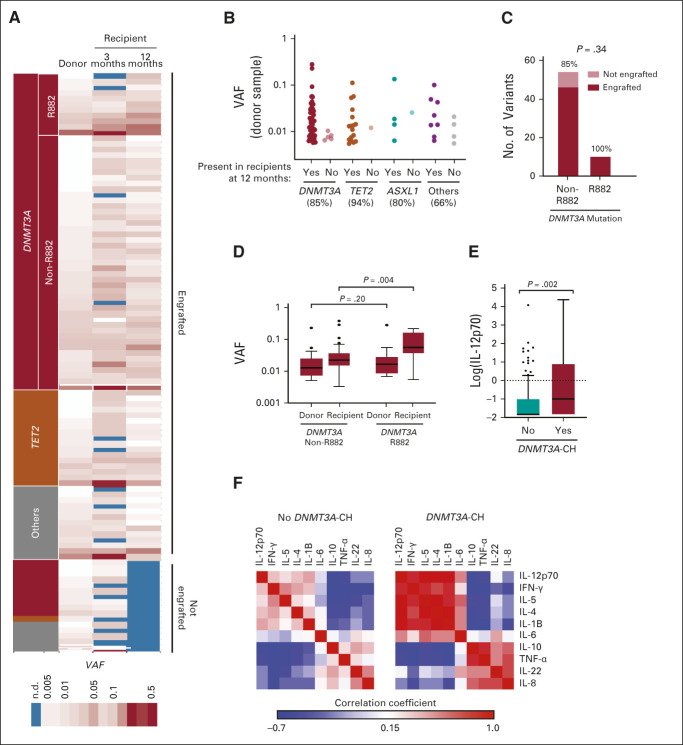
We performed targeted error-corrected sequencing on samples from 1,727 donors age 40 years or older and assessed the effect of donor CH on recipient clinical outcomes. We measured long-term engraftment of 102 donor clones and cytokine levels in 256 recipients at 3 and 12 months after transplant.
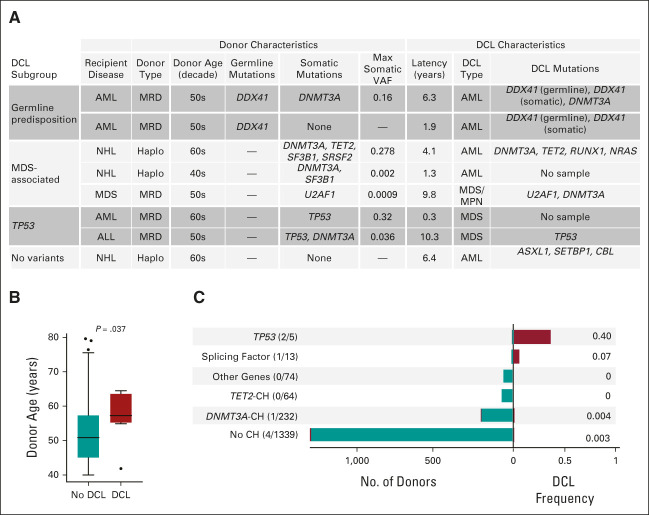
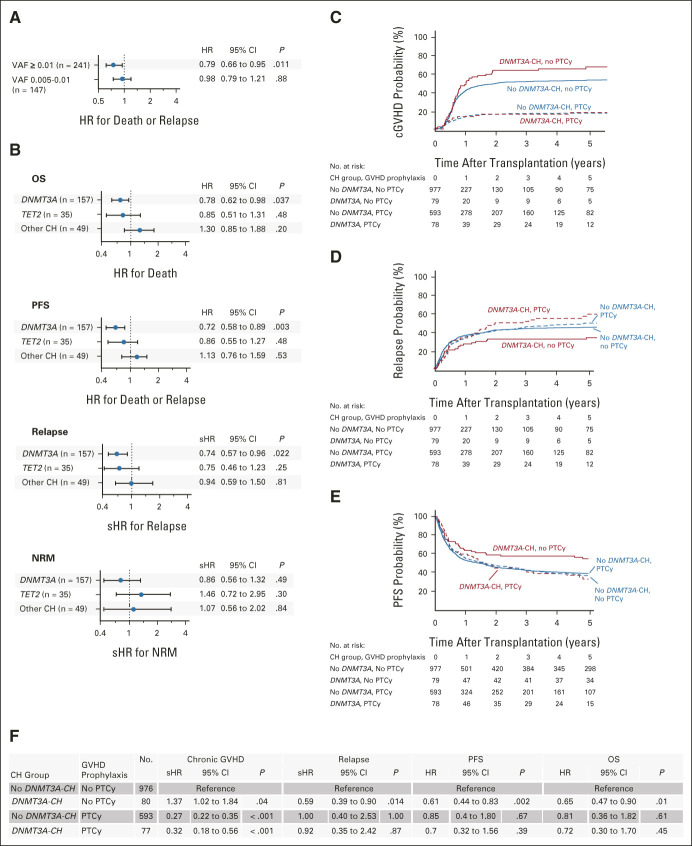
CH was present in 22.5% of donors, with (14.6%) and (5.2%) mutations being most common; 85% of donor clones showed long-term engraftment in recipients after transplantation, including clones with a variant allele fraction < 0.01. CH with a variant allele fraction ≥ 0.01, but not smaller clones, was associated with improved recipient overall (hazard ratio [HR], 0.79; = .042) and progression-free survival (HR, 0.72; = .003) after adjustment for significant clinical variables. In patients who received calcineurin-based graft-versus-host disease prophylaxis, donor CH was associated with reduced relapse (subdistribution HR, 0.59; = .014), increased chronic graft-versus-host disease (subdistribution HR, 1.36; = .042), and higher interleukin-12p70 levels in recipients. No recipient of sole or -CH developed donor cell leukemia (DCL). In seven of eight cases, DCL evolved from donor CH with rare or splicing factor mutations or from donors carrying germline mutations.
Donor CH is closely associated with clinical outcomes in transplant recipients, with differential impact on graft alloimmune function and potential for leukemic transformation related to mutated gene and somatic clonal abundance. Donor -CH is associated with improved recipient survival because of reduced relapse risk and with an augmented network of inflammatory cytokines in recipients. Risk of DCL in allogeneic hematopoietic cell transplantation is driven by somatic myelodysplastic syndrome-associated mutations or germline predisposition in donors.
在异基因造血细胞移植中,克隆性造血(CH)可从供体传播给受体。由于其对受体结局和移植物同种免疫功能的影响尚不确定,因此排除具有 CH 的候选供体存在争议。
我们对 1727 名年龄在 40 岁或以上的供体样本进行了靶向纠错测序,并评估了供体 CH 对受体临床结局的影响。我们测量了 256 名受体在移植后 3 个月和 12 个月时 102 个供体克隆的长期植入情况和细胞因子水平。
22.5%的供体存在 CH,最常见的突变是 (14.6%)和 (5.2%);85%的供体克隆在移植后在受体中表现出长期植入,包括等位基因变异分数<0.01 的克隆。具有等位基因变异分数≥0.01 的 CH,但不是较小的克隆,与调整重要临床变量后受体的总生存率(风险比[HR],0.79;P=.042)和无进展生存率(HR,0.72;P=.003)的改善相关。在接受钙调神经磷酸酶为基础的移植物抗宿主病预防的患者中,供体 CH 与降低复发相关(亚分布 HR,0.59;P=.014),增加慢性移植物抗宿主病(亚分布 HR,1.36;P=.042),以及受体中白细胞介素-12p70 水平升高。没有受体仅发生 或 -CH 发展为供体细胞白血病(DCL)。在 8 例中的 7 例中,DCL 是由供体 CH 发展而来,伴有罕见的 或剪接因子突变,或由携带胚系 突变的供体引起。
供体 CH 与移植受者的临床结局密切相关,对移植物同种免疫功能的影响不同,并且与突变基因和体细胞克隆丰度相关的白血病转化的可能性相关。由于复发风险降低,供体 -CH 与受体生存改善相关,并且受体中炎症细胞因子网络增强。异基因造血细胞移植中 DCL 的风险是由供体中的体细胞骨髓增生异常综合征相关突变或胚系易感性驱动的。