Dana-Farber Cancer Institute, Boston, Massachusetts, USA
Harvard Medical School, Boston, Massachusetts, USA.
J Immunother Cancer. 2021 Nov;9(11). doi: 10.1136/jitc-2021-003743.
Treatment-free survival (TFS) characterizes disease control after discontinuation of immune checkpoint inhibitors (ICIs) until subsequent therapy or death. We previously evaluated TFS in a pooled analysis of the CheckMate 067 and CheckMate 069 trials of the ICIs nivolumab and ipilimumab, alone or in combination, in patients with advanced melanoma after minimum follow-up of 36 months. This analysis investigated TFS differences between treatments in CheckMate 067 after a minimum follow-up of 60 months, and their relation to overall survival (OS) differences.
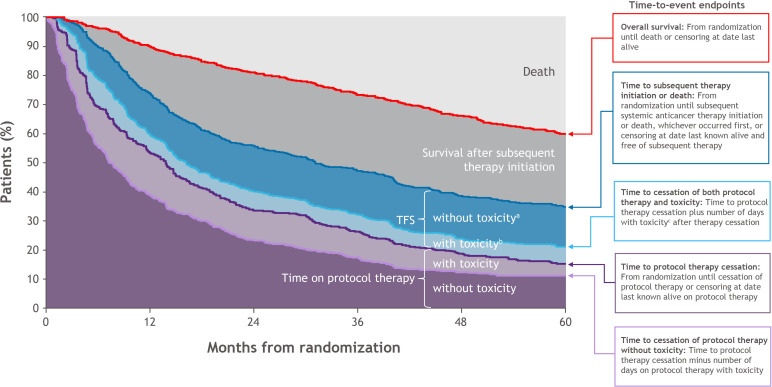
Data were from 937 patients who initiated treatment (nivolumab plus ipilimumab, nivolumab, or ipilimumab) in CheckMate 067 (NCT01844505). TFS was defined as the area between the Kaplan-Meier curves for time to protocol therapy cessation and time to subsequent systemic therapy initiation or death, each measured from randomization. TFS was partitioned as time with and without toxicity. Toxicity included persistent and late-onset grade ≥2 select treatment-related adverse events (ie, those of potential immunologic etiology). The area between Kaplan-Meier curves was estimated by the difference in 60-month restricted-mean times of the endpoints. Between-group differences were estimated with bootstrapped 95% CIs.
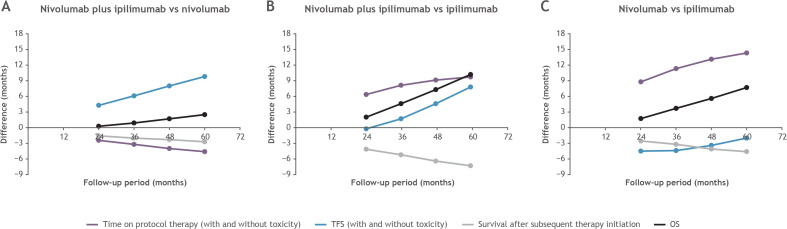
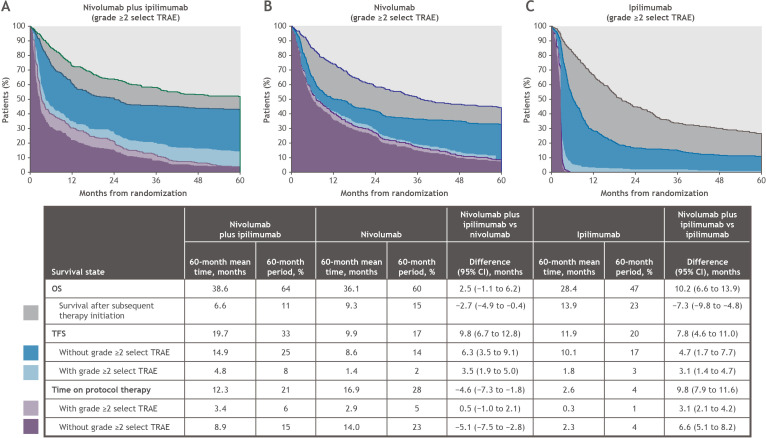
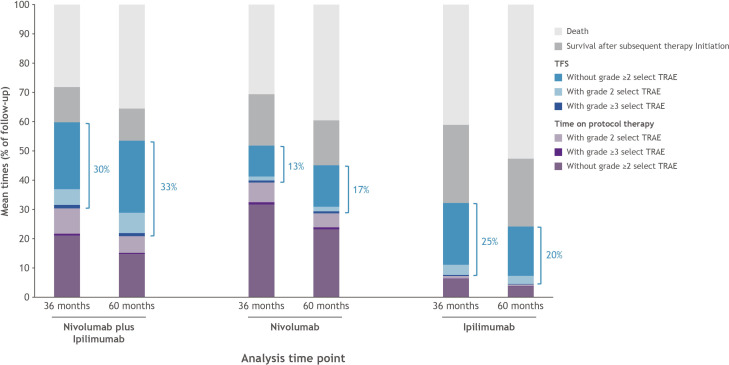
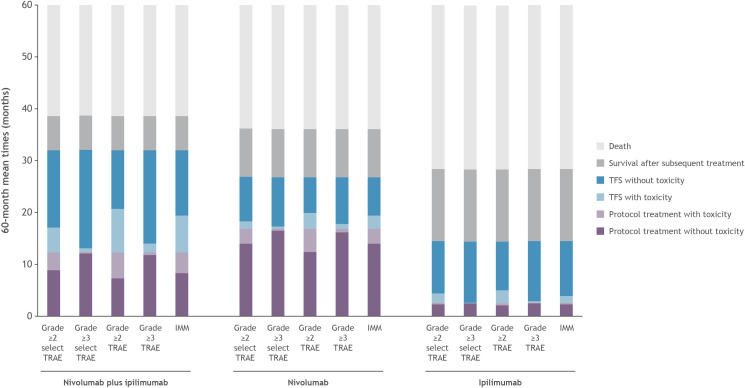
At 60 months from randomization, 39%, 24%, and 11% of patients assigned to treatment with nivolumab plus ipilimumab, nivolumab, and ipilimumab, respectively, had survived and were treatment-free. The 60-month mean TFS was approximately twice as long with the combination (19.7 months) than with nivolumab (9.9 months; absolute difference, 9.8 (95% CI 6.7 to 12.8)) or ipilimumab (11.9 months; absolute difference, 7.8 (95% CI 4.6 to 11.0)). In the respective groups, mean TFS represented 33% (8% with and 25% without toxicity), 17% (2% and 14%), and 20% (3% and 17%) of the 60-month period. Compared with 36-month estimates, mean TFS over the 60-month period represented slightly greater percentages of time in the nivolumab-containing regimen groups and a lesser percentage in the ipilimumab group. TFS differences between the combination and either monotherapy increased with longer follow-up.
Along with improved long-term OS with the nivolumab-containing regimens versus ipilimumab, TFS without toxicity was sustained with nivolumab plus ipilimumab versus either monotherapy, demonstrating larger between-group differences with extended follow-up.
在免疫检查点抑制剂(ICI)停药后直至后续治疗或死亡期间,无治疗生存(TFS)可用于评估疾病的控制情况。我们之前对纳武单抗和伊匹单抗单药或联合治疗晚期黑色素瘤患者的 CheckMate 067 和 CheckMate 069 试验进行了汇总分析,在至少 36 个月的随访后评估了 TFS。本分析在 CheckMate 067 中研究了至少 60 个月随访后不同治疗组之间 TFS 的差异及其与总生存期(OS)差异的关系。
本研究的数据来自 937 例患者,这些患者在 CheckMate 067 中开始接受治疗(纳武单抗联合伊匹单抗、纳武单抗或伊匹单抗)(NCT01844505)。TFS 定义为从随机分组到方案治疗终止时间和随后系统治疗开始或死亡时间之间的 Kaplan-Meier 曲线之间的区域,每个时间点均从随机分组开始测量。TFS 分为有和无毒性的时间。毒性包括持续性和迟发性 2 级及以上选择治疗相关不良事件(即具有潜在免疫病因的不良事件)。通过终点 60 个月限制均值时间的差异估计 Kaplan-Meier 曲线之间的区域。使用 bootstrap 95%CI 估计组间差异。
从随机分组到 60 个月时,分别有 39%、24%和 11%接受纳武单抗联合伊匹单抗、纳武单抗和伊匹单抗治疗的患者存活且无治疗。联合治疗(19.7 个月)的 60 个月平均 TFS 大约是纳武单抗(9.9 个月;绝对差异 9.8(95%CI 6.7 至 12.8))或伊匹单抗(11.9 个月;绝对差异 7.8(95%CI 4.6 至 11.0))的两倍。在各自的组中,60 个月的平均 TFS 分别代表 33%(8%有和 25%无毒性)、17%(2%有和 14%无毒性)和 20%(3%有和 17%无毒性)。与 36 个月的估计值相比,纳武单抗组的 TFS 在 60 个月期间代表的时间百分比略有增加,而伊匹单抗组的百分比则略有下降。随着随访时间的延长,联合治疗与单药治疗之间的 TFS 差异增加。
与伊匹单抗相比,纳武单抗联合治疗方案的长期 OS 得到改善,而无毒性的 TFS 在纳武单抗联合伊匹单抗与单药治疗中持续存在,随着随访时间的延长,组间差异更大。