Dana-Farber Cancer Institute, Boston, MA.
Harvard Medical School, Boston, MA.
J Clin Oncol. 2019 Dec 10;37(35):3350-3358. doi: 10.1200/JCO.19.00345. Epub 2019 Sep 9.
Outcome measures that comprehensively capture attributes of immuno-oncology agents, including prolonged treatment-free time and persistent treatment-related adverse events (TRAEs), are needed to complement conventional survival end points.
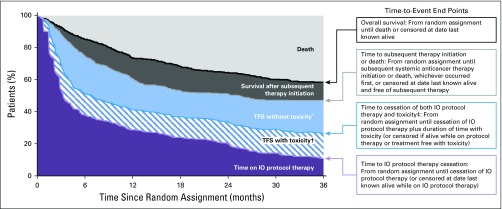
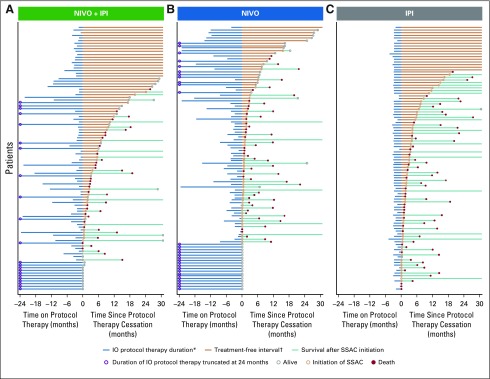
We pooled data from the CheckMate 067 and 069 clinical trials of nivolumab and ipilimumab, as monotherapies or in combination, for patients with advanced melanoma. Treatment-free survival (TFS) was defined as the area between Kaplan-Meier curves for two conventional time-to-event end points, each defined from random assignment: time to immune checkpoint inhibitor (ICI) protocol therapy cessation and time to subsequent systemic therapy initiation or death. TFS was partitioned as time with and without toxicity by a third end point, time to cessation of both ICI therapy and toxicity. Toxicity included persistent and late-onset grade 3 or higher TRAEs. The area under each Kaplan-Meier curve was estimated by the 36-month restricted mean time.
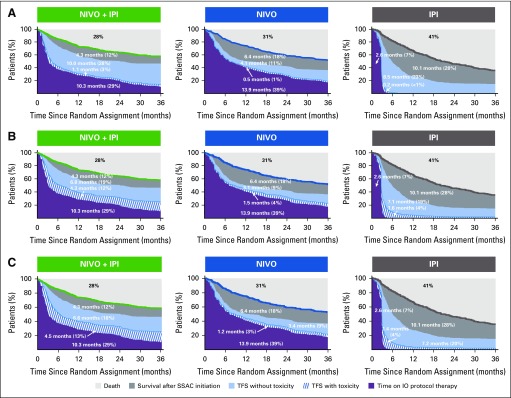
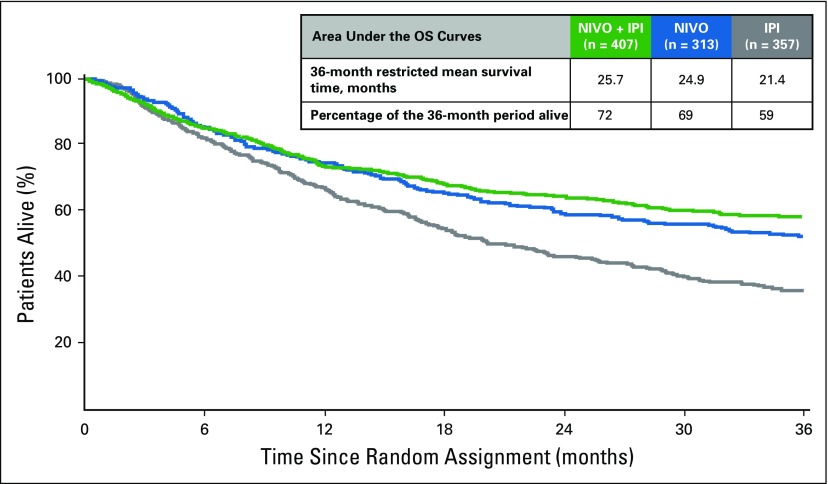
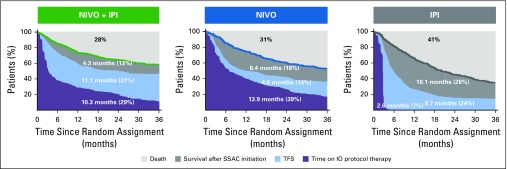
At 36 months, many of the 1,077 patients who initiated ICI therapy were surviving free of subsequent therapy initiation (47% nivolumab plus ipilimumab, 37% nivolumab, 15% ipilimumab). The restricted mean TFS was longer for nivolumab plus ipilimumab (11.1 months) compared with nivolumab (4.6 months; difference, 6.5 months; 95% CI, 5.0 to 8.0 months) or ipilimumab (8.7 months; difference, 2.4 months; 95% CI, 0.8 to 4.1 months); restricted mean TFS represented 31% (3% with and 28% without toxicity), 13% (1% and 11%), and 24% (less than 1% and 23%) of the 36-month period, respectively, in the three treatment groups. TFS without toxicity was longer for nivolumab plus ipilimumab than nivolumab (difference, 6.0 months) or ipilimumab (difference, 1.7 months).
The analysis of TFS between ICI cessation and subsequent therapy initiation revealed longer TFS without toxicity for patients with advanced melanoma who received nivolumab plus ipilimumab compared with nivolumab or ipilimumab. Regardless of treatment, a small proportion of the TFS involved grade 3 or higher TRAEs.
需要能够全面捕捉免疫肿瘤药物属性的疗效指标,包括延长无治疗时间和持续的治疗相关不良反应(TRAEs),以补充传统的生存终点。
我们对纳武单抗和伊匹单抗单药或联合治疗晚期黑色素瘤患者的 CheckMate 067 和 069 临床试验数据进行了汇总。无治疗生存期(TFS)定义为两条常规时间至事件终点曲线之间的区域,每个终点均从随机分组开始定义:免疫检查点抑制剂(ICI)方案治疗停药时间和随后开始系统治疗或死亡时间。TFS 通过第三个终点,ICI 治疗和毒性停止时间,分为有和无毒性的两个部分。毒性包括持续性和迟发性 3 级或更高 TRAEs。每条 Kaplan-Meier 曲线下的面积通过 36 个月限制平均时间来估计。
在 36 个月时,许多开始 ICI 治疗的 1077 名患者中有许多在没有后续治疗的情况下存活下来(47%纳武单抗联合伊匹单抗,37%纳武单抗,15%伊匹单抗)。纳武单抗联合伊匹单抗的限制性平均 TFS 长于纳武单抗(11.1 个月)(差异为 6.5 个月;95%CI,5.0 至 8.0 个月)或伊匹单抗(8.7 个月;差异为 2.4 个月;95%CI,0.8 至 4.1 个月);限制平均 TFS 分别代表三个治疗组中 36 个月期间的 31%(有和无毒性各 3%)、13%(有和无毒性各 1%)和 24%(小于 1%和 23%)。纳武单抗联合伊匹单抗的无毒性 TFS 长于纳武单抗(差异为 6.0 个月)或伊匹单抗(差异为 1.7 个月)。
ICI 停药与后续治疗开始之间的 TFS 分析显示,与纳武单抗或伊匹单抗相比,接受纳武单抗联合伊匹单抗治疗的晚期黑色素瘤患者无毒性 TFS 更长。无论治疗如何,TFS 的一小部分涉及 3 级或更高 TRAEs。