Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA.
Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA; Department of Medicine, Emory University School of Medicine, Atlanta, Georgia, USA.
JACC Cardiovasc Imaging. 2022 Mar;15(3):489-500. doi: 10.1016/j.jcmg.2021.09.018. Epub 2021 Nov 17.
This study sought to assess the relationship between mean vs peak calcified plaque density and their impact on calculating coronary artery calcium (CAC) scores and to compare the corresponding differential prediction of atherosclerotic cardiovascular disease (ASCVD) and coronary heart disease (CHD) mortality.
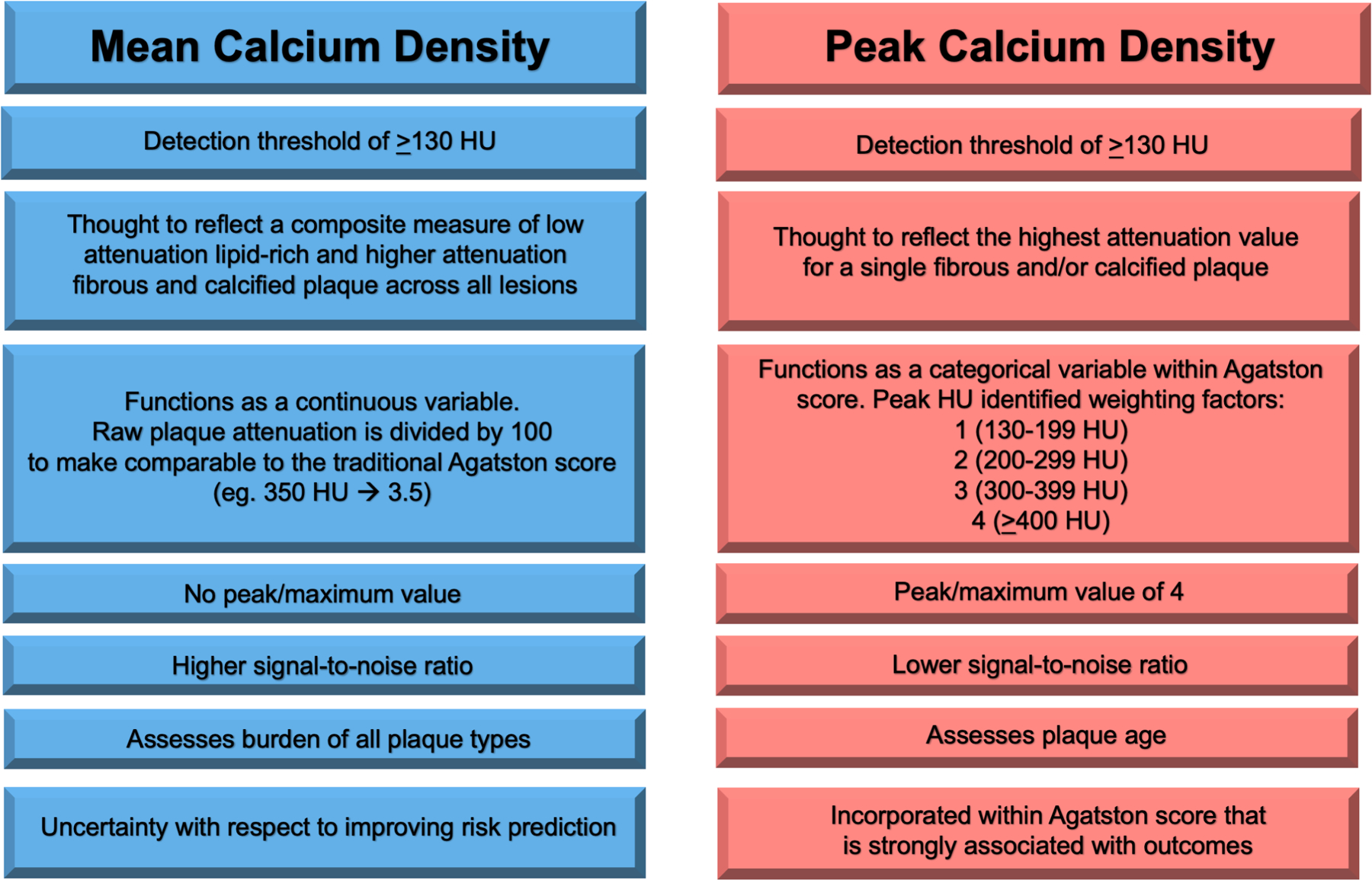
The Agatston CAC score is quantified per lesion as the product of plaque area and a 4-level categorical peak calcium density factor. However, mean calcium density may more accurately measure the heterogenous mixture of lipid-rich, fibrous, and calcified plaque reflective of ASCVD risk.
We included 10,373 individuals from the CAC Consortium who had CAC >0 and per-vessel measurements of peak calcium density factor and mean calcium density. Area under the curve and continuous net reclassification improvement analyses were performed for CHD and ASCVD mortality to compare the predictive abilities of mean calcium density vs peak calcium density factor when calculating the Agatston CAC score.
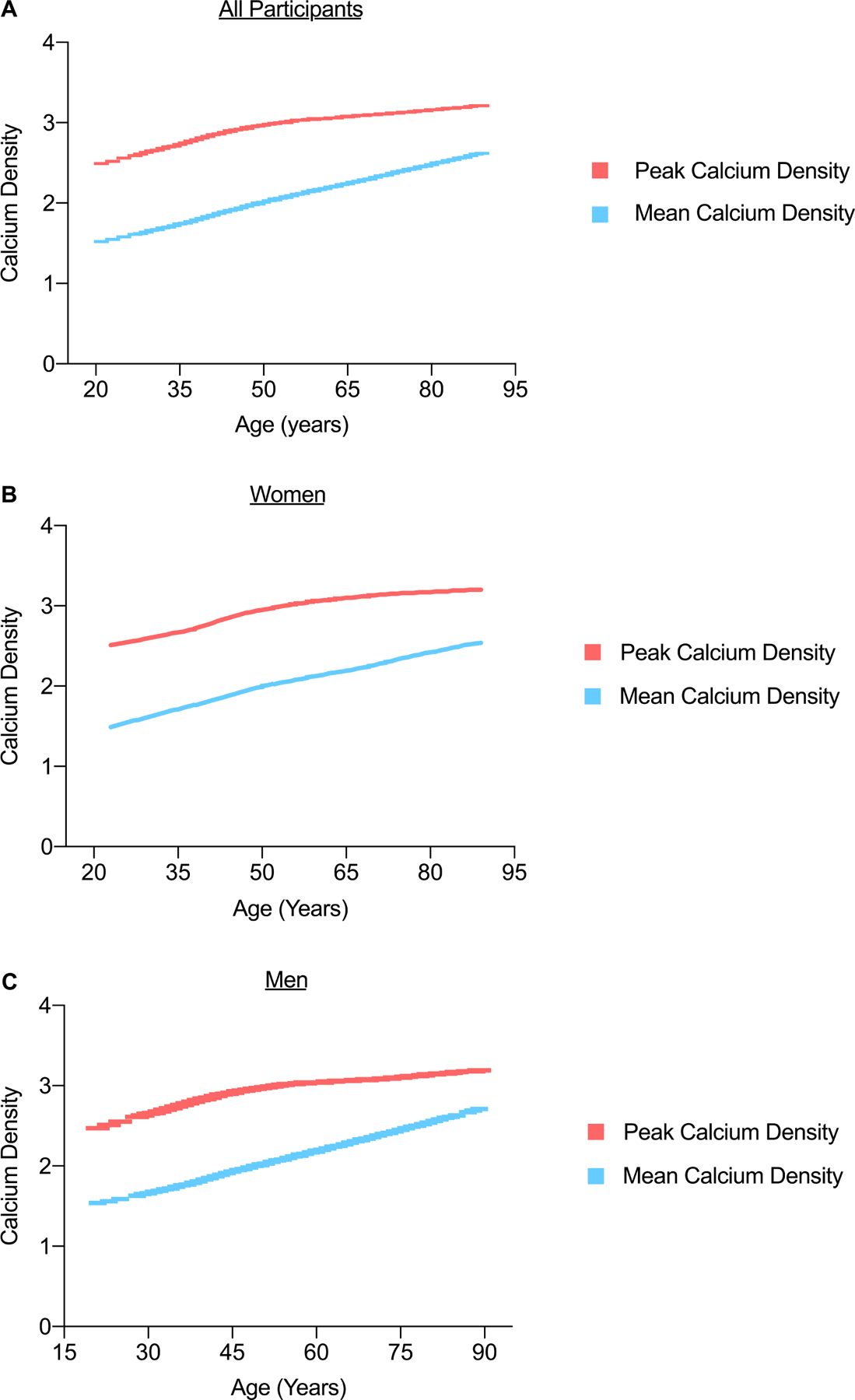
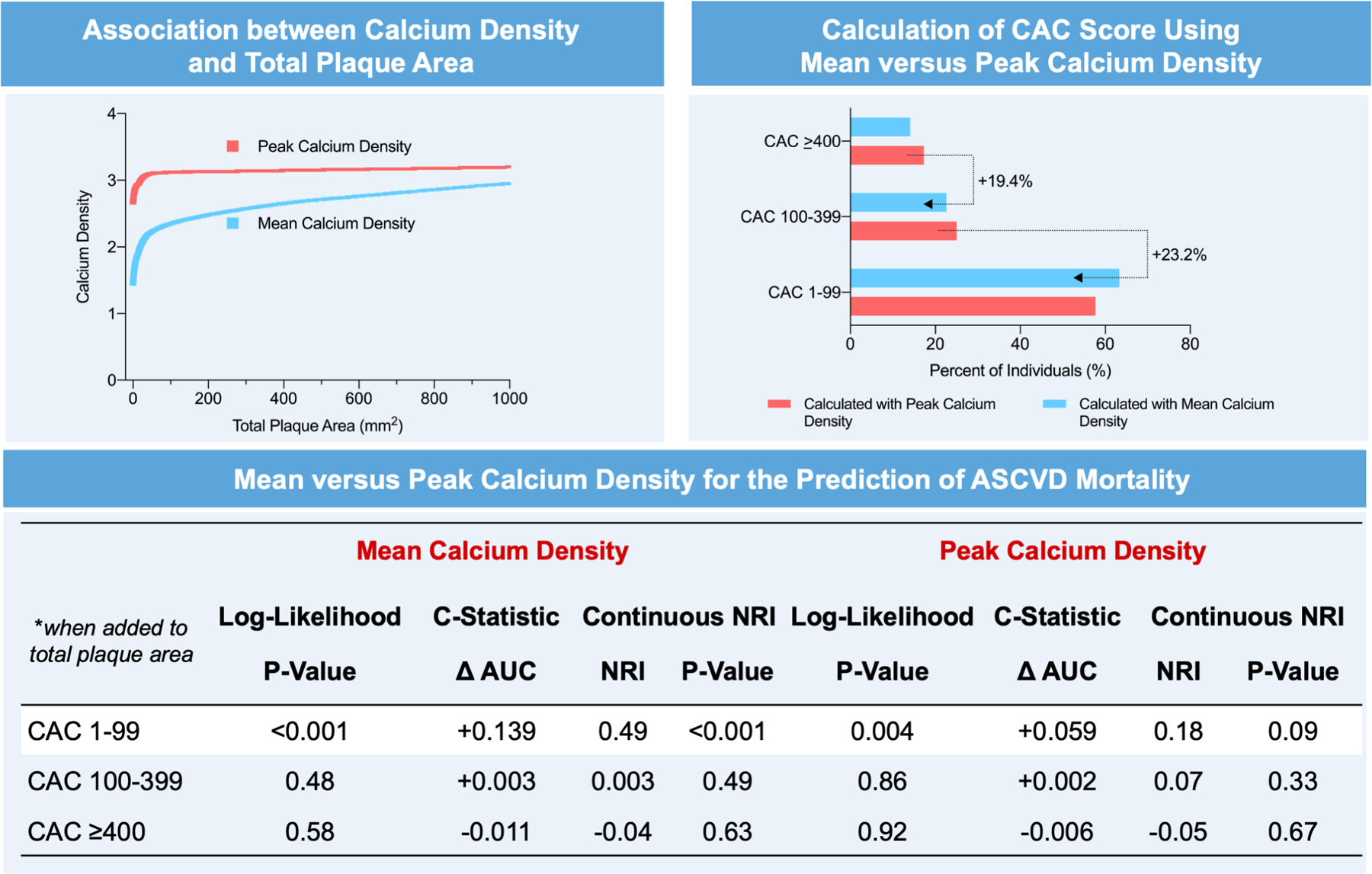
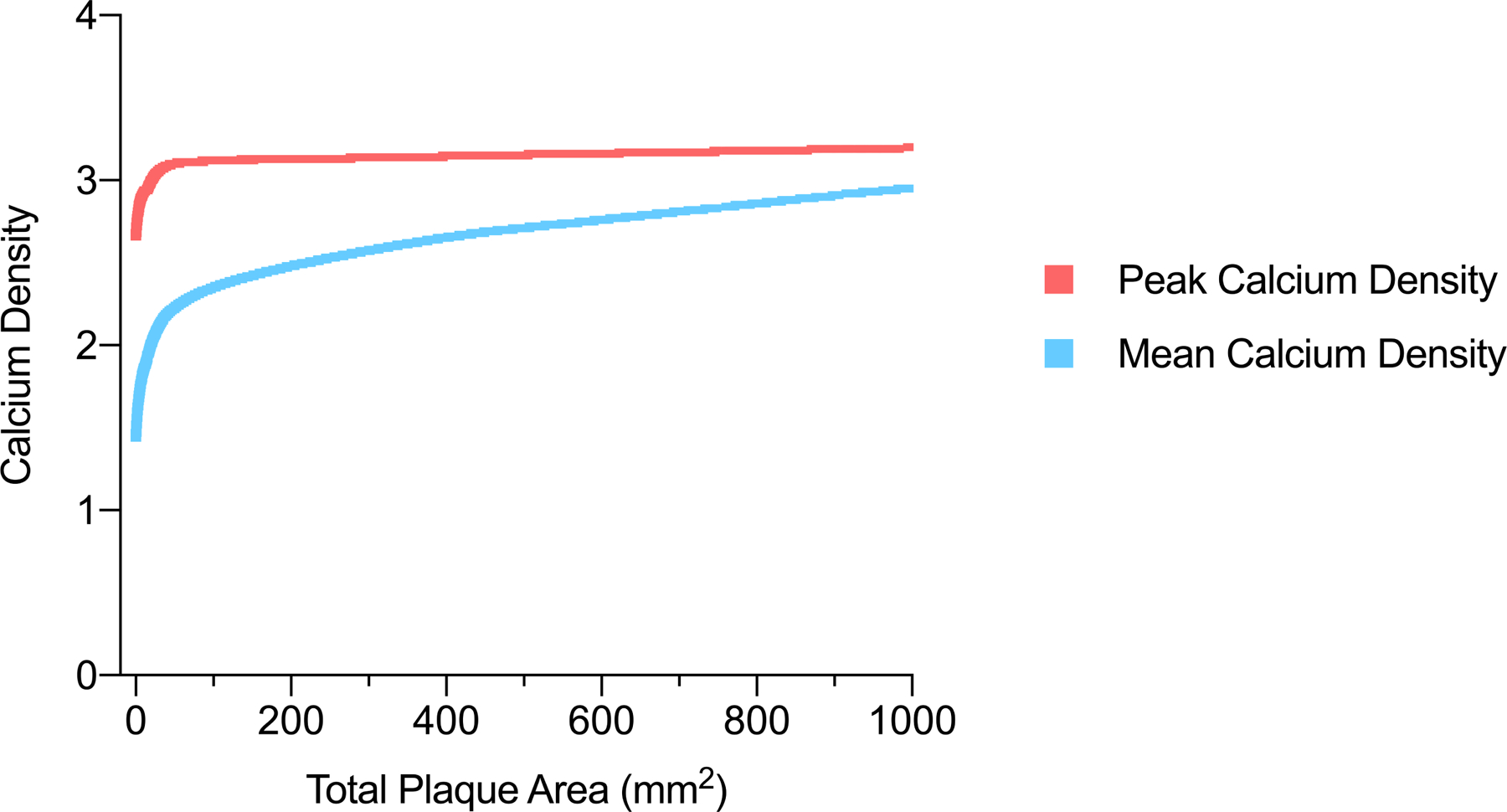
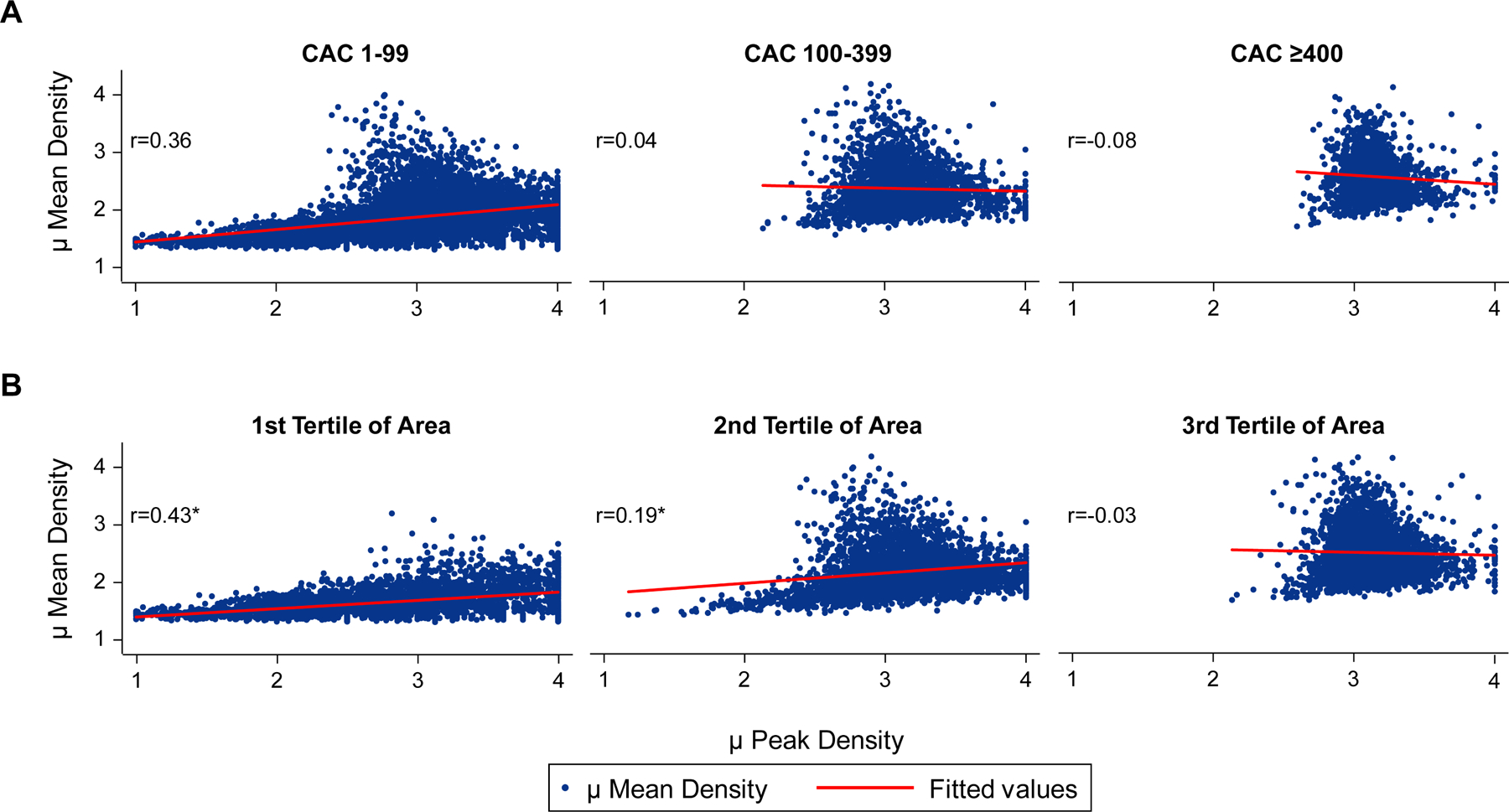
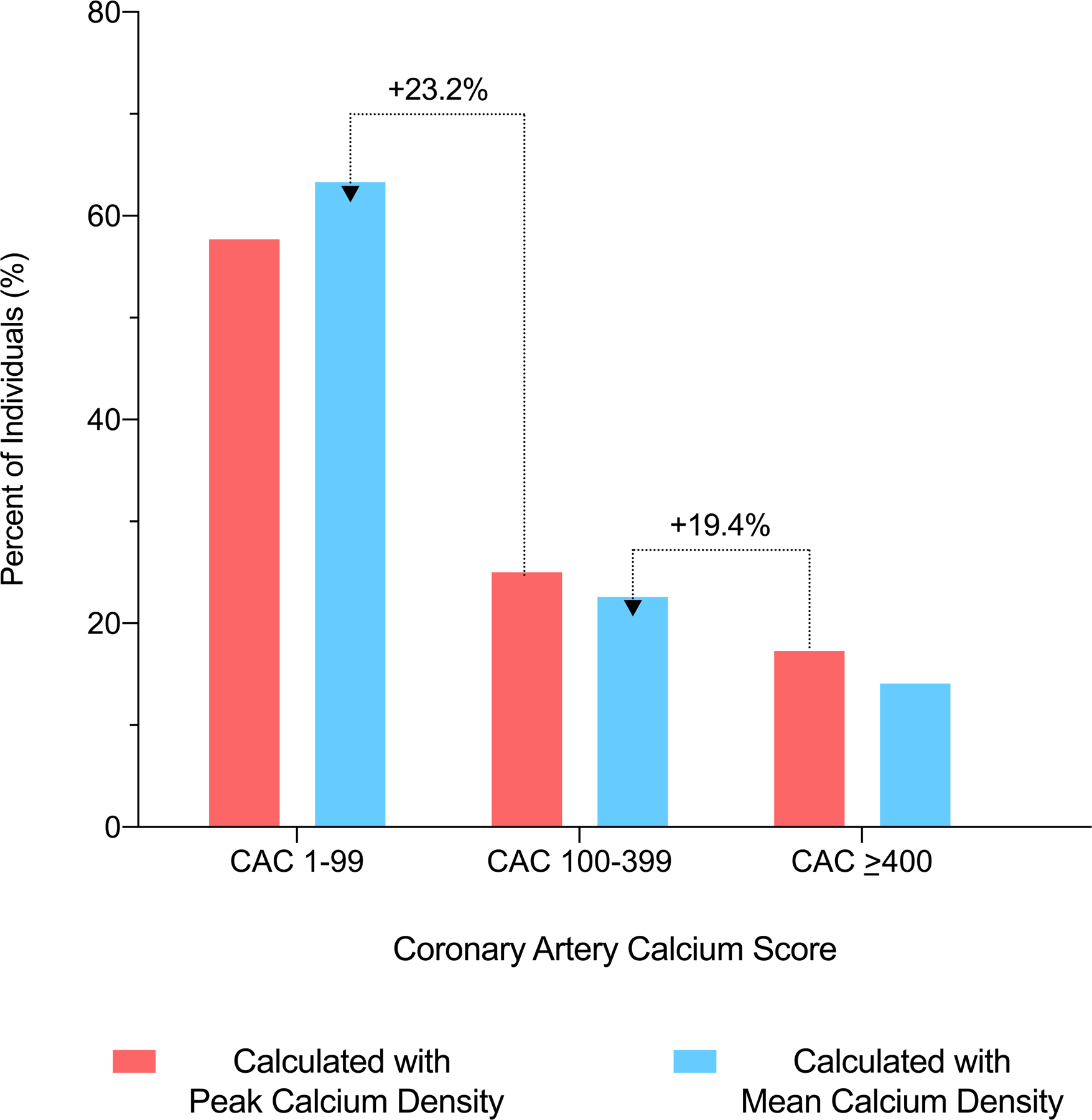
Participants were on average 53.4 years of age, 24.4% were women, and the median CAC score was 68 Agatston units. The average values for mean calcium density and peak calcium density factor were 210 ± 50 HU and 3.1 ± 0.5, respectively. Individuals younger than 50 years of age and/or those with a total plaque area <100 mm had the largest differences between the peak and mean density measures. Among persons with CAC 1-99, the use of mean calcium density resulted in a larger improvement in ASCVD mortality net reclassification improvement (NRI) (NRI = 0.49; P < 0.001 vs. NRI = 0.18; P = 0.08) and CHD mortality discrimination (Δ area under the curve (AUC) = +0.169 vs +0.036; P < 0.001) compared with peak calcium density factor. Neither peak nor mean calcium density improved mortality prediction at CAC scores >100.
Mean and peak calcium density may differentially describe plaque composition early in the atherosclerotic process. Mean calcium density performs better than peak calcium density factor when combined with plaque area for ASCVD mortality prediction among persons with Agatston CAC 1-99.
本研究旨在评估平均钙化斑块密度与峰值钙化斑块密度之间的关系及其对计算冠状动脉钙(CAC)评分的影响,并比较其对动脉粥样硬化性心血管疾病(ASCVD)和冠心病(CHD)死亡率的预测差异。
Agatston CAC 评分按病变计算,乘积为斑块面积和 4 级分类的峰值钙密度因子。然而,平均钙密度可能更准确地测量富含脂质、纤维和钙化斑块的异质混合物,反映 ASCVD 风险。
我们纳入了 CAC 联合会的 10373 名 CAC>0 且有血管内峰值钙密度因子和平均钙密度测量值的个体。进行曲线下面积和连续净重新分类改进分析,以比较在计算 Agatston CAC 评分时,平均钙密度与峰值钙密度因子对 CHD 和 ASCVD 死亡率的预测能力。
参与者平均年龄为 53.4 岁,24.4%为女性,中位 CAC 评分为 68 个 Agatston 单位。平均钙密度和峰值钙密度因子值分别为 210±50HU 和 3.1±0.5。年龄<50 岁和/或总斑块面积<100mm 的个体,其峰值和平均密度值之间的差异最大。在 CAC 为 1-99 的个体中,使用平均钙密度可显著提高 ASCVD 死亡率净重新分类改进(NRI)(NRI=0.49;P<0.001 vs. NRI=0.18;P=0.08)和 CHD 死亡率判别(Δ曲线下面积(AUC)=+0.169 vs.+0.036;P<0.001),与峰值钙密度因子相比。在 CAC 评分>100 时,峰值和平均钙密度均不能改善死亡率预测。
平均和峰值钙密度可能在动脉粥样硬化过程早期不同程度地描述斑块组成。在 Agatston CAC 为 1-99 的个体中,当与斑块面积结合使用时,平均钙密度对 ASCVD 死亡率的预测优于峰值钙密度因子。