Castellucci Andrea, Botti Cecilia, Martellucci Salvatore, Malara Pasquale, Delmonte Silvia, Lusetti Francesca, Ghidini Angelo
ENT Unit, Department of Surgery, Azienda USL-IRCCS di Reggio Emilia, Reggio Emilia, Italy.
PhD Program in Clinical and Experimental Medicine, University of Modena and Reggio Emilia, Modena, Italy.
J Audiol Otol. 2022 Jul;26(3):153-159. doi: 10.7874/jao.2021.00297. Epub 2021 Nov 23.
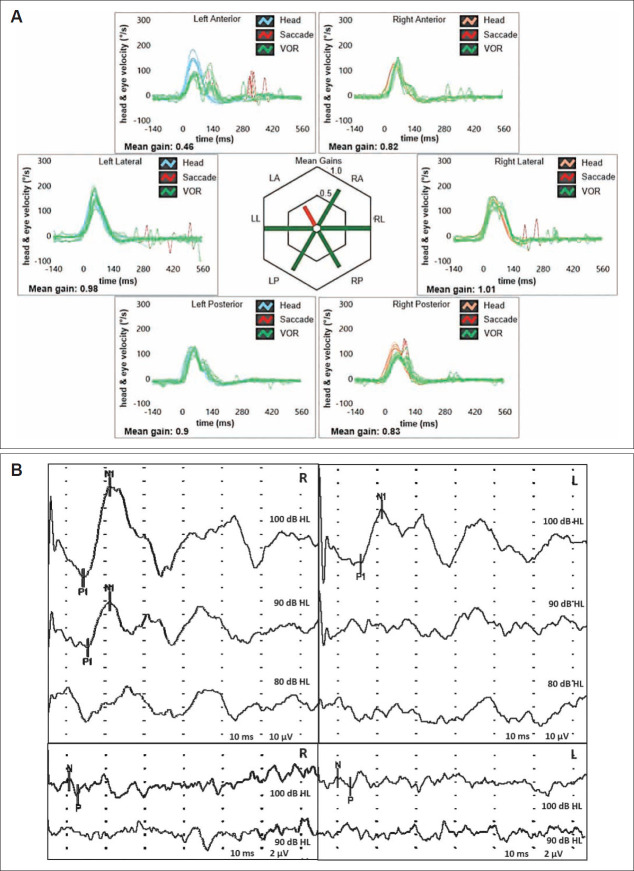
We describe a rare case of spontaneous upbeat nystagmus (UBN) attributable to a canalith jam involving the anterior semicircular canal (ASC) in a patient in whom comprehensive vestibular assessment was useful to identify the underlying pathomechanism. A 56-year-old woman with unsteadiness following repositioning procedures for left-sided benign paroxysmal positional vertigo (BPPV) presented with spontaneous UBN that showed slight right torsional components. A vestibular test battery detected isolated left ASC hypofunction on a video-head impulse test (Video-HIT). We postulated a persistent utriculopetal deflection of the left ASC cupula, which was attributable to entrapment of debris in a narrow canal tract, with consequent sustained inhibition of the ampullary afferents. Although spontaneous UBN receded after impulsive physical therapy, unsteadiness deteriorated into positional vertigo secondary to canalolithiasis involving the ipsilateral posterior canal. In our view, physical therapy possibly fragmented the canalith jam and released free-floating otoconia that eventually settled into the ipsilateral posterior canal. Video HIT revealed normalization of ASC hypofunction, and leftsided posterior canal canalolithiasis was successfully treated using appropriate repositioning procedures. We propose that a canalith jam involving the ASC should be considered in the differential diagnosis of spontaneous UBN, particularly in patients with a history of BPPV and isolated ASC hypofunction detected on video HIT.
我们描述了一例罕见的自发性上跳性眼震(UBN)病例,其病因是一名患者的前半规管(ASC)出现嵴帽结石嵌顿,全面的前庭评估有助于确定潜在的发病机制。一名56岁女性在接受左侧良性阵发性位置性眩晕(BPPV)复位治疗后出现不稳,并伴有自发性UBN,有轻微的右扭转成分。前庭检查发现视频头脉冲试验(Video-HIT)显示孤立的左侧ASC功能减退。我们推测左侧ASC壶腹嵴持续向椭圆囊偏斜,这是由于碎片被困在狭窄的管腔内,导致壶腹传入神经持续受到抑制。尽管在进行冲动性物理治疗后自发性UBN有所减轻,但不稳症状恶化为同侧后半规管管石症继发的位置性眩晕。我们认为,物理治疗可能使嵴帽结石嵌顿破碎,释放出自由漂浮的耳石,最终沉积在同侧后半规管。视频HIT显示ASC功能减退恢复正常,采用适当的复位程序成功治疗了左侧后半规管管石症。我们建议,在自发性UBN的鉴别诊断中,应考虑ASC嵴帽结石嵌顿的情况,特别是对于有BPPV病史且视频HIT检测到孤立的ASC功能减退的患者。