Department of Medicine, University of Alabama at Birmingham, Birmingham, AL, United States of America.
Department of Pathology, University of Alabama at Birmingham, Birmingham, AL, United States of America.
PLoS One. 2021 Nov 23;16(11):e0260345. doi: 10.1371/journal.pone.0260345. eCollection 2021.
No medical treatment has proven efficacy for acute exacerbations of idiopathic pulmonary fibrosis (AE-IPF), and this syndrome has a very high mortality. Based on data indicating humoral autoimmune processes are involved in IPF pathogenesis, we treated AE-IPF patients with an autoantibody reduction regimen of therapeutic plasma exchange, rituximab, and intravenous immunoglobulin. This study aimed to identify clinical and autoantibody determinants associated with survival after autoantibody reduction in AE-IPF.
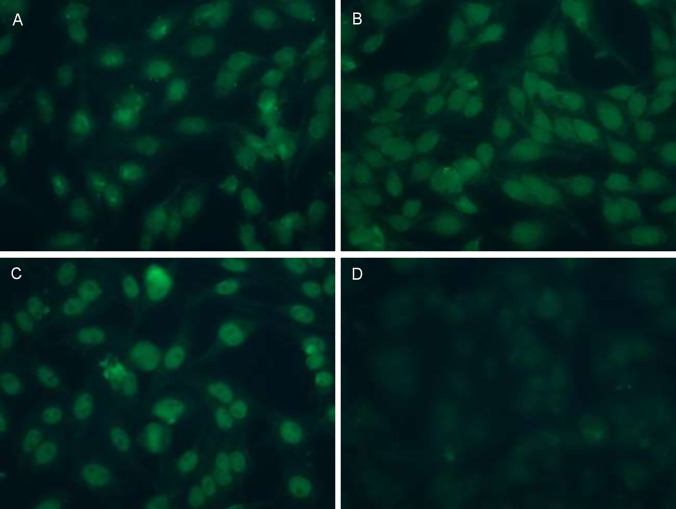
Twenty-four(24) AE-IPF patients received the autoantibody reduction regimen. Plasma anti-epithelial autoantibody titers were determined by HEp-2 indirect immunofluorescence assays in 22 patients.
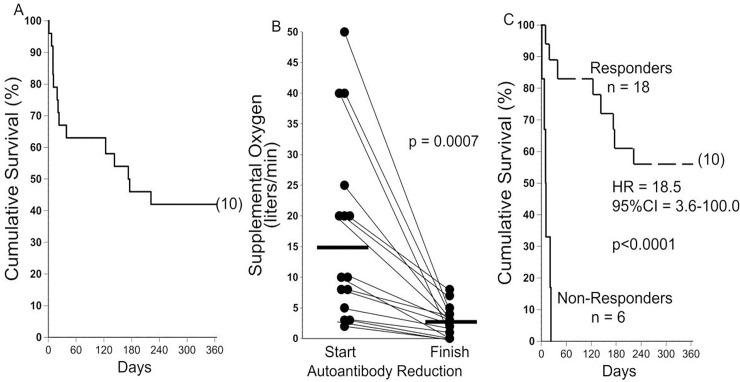
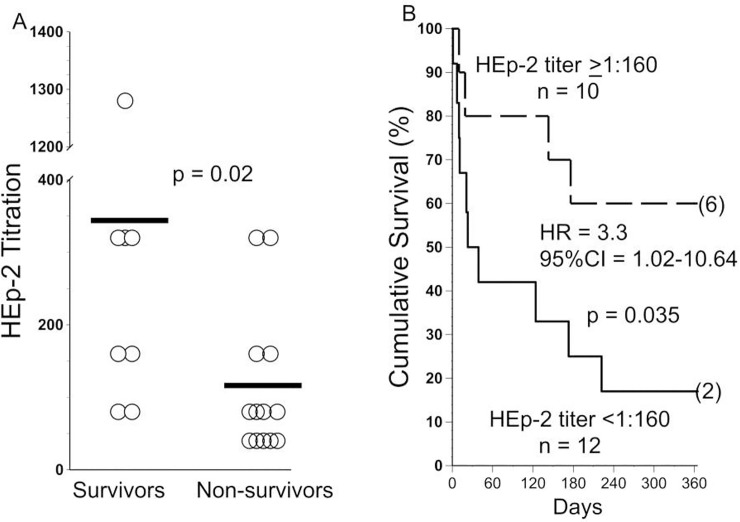
Mean age of the patients was 70 + 7 years old, and 70% were male. Beneficial clinical responses that occurred early during therapy were a favorable prognostic indicator: supplemental O2 flows needed to maintain resting SaO2>92% significantly decreased and/or walk distances increased among all 10 patients who survived for at least one year. Plasma anti-HEp-2 autoantibody titers were ~-three-fold greater in survivors compared to non-survivors (p<0.02). Anti-HEp-2 titers >1:160 were present in 75% of the evaluable one-year survivors, compared to 29% of non-survivors, and 10 of 12 patients (83%) with anti-HEP-2 titers <1:160 died during the observation period (Hazard Ratio = 3.3, 95% Confidence Interval = 1.02-10.6, p = 0.047).
Autoantibody reduction therapy is associated with rapid reduction of supplemental oxygen requirements and/or improved ability to ambulate in many AE-IPF patients. Facile anti-epithelial autoantibody assays may help identify those most likely to benefit from these treatments.
尚无医学疗法可有效治疗特发性肺纤维化急性加重(AE-IPF),且该综合征的死亡率极高。基于表明体液自身免疫过程与 IPF 发病机制相关的数据,我们采用治疗性血浆置换、利妥昔单抗和静脉注射免疫球蛋白的自身抗体降低方案治疗 AE-IPF 患者。本研究旨在确定与 AE-IPF 患者接受自身抗体降低治疗后的生存相关的临床和自身抗体决定因素。
24 例 AE-IPF 患者接受了自身抗体降低方案治疗。通过间接免疫荧光法在 22 例患者中测定血浆抗上皮自身抗体滴度。
患者的平均年龄为 70+7 岁,70%为男性。治疗早期发生的有益临床反应是一个有利的预后指标:所有至少存活 1 年的 10 例患者的静息 SaO2>92%所需的补充氧气流量显著降低,并且/或者行走距离增加。与非幸存者相比,幸存者的血浆抗 HEp-2 自身抗体滴度高约 3 倍(p<0.02)。在可评估的 1 年幸存者中,75%的患者存在抗-HEp-2 滴度>1:160,而非幸存者为 29%,12 例患者中的 10 例(83%)抗-HEP-2 滴度<1:160 在观察期间死亡(风险比=3.3,95%置信区间=1.02-10.6,p=0.047)。
自身抗体降低治疗与许多 AE-IPF 患者补充氧气需求的快速降低和/或步行能力的改善相关。上皮自身抗体的简便检测可能有助于识别最有可能从这些治疗中受益的患者。