Unity Health Toronto and the Li Ka Shing Knowledge Institute (Gomes, Kitchen, Mamdani), St. Michael's Hospital; ICES (Gomes, McCormack, Paterson, Mamdani, Tadrous); Canada; Institute for Health Policy, Management, and Evaluation (Gomes, Paterson, Mamdani), and the Leslie Dan Faculty of Pharmacy (Gomes, Mamdani, Tadrous) at the University of Toronto, Toronto, Ont.; Department of Family Medicine (Paterson), McMaster University, Hamilton, Ont.; Women's College Hospital (Tadrous), Ontario Drug Policy Research Network (Gomes, McCormack, Kitchen, Paterson, Mamdani, Proulx, Bayliss, Tadrous), Toronto, Ont.
CMAJ Open. 2021 Nov 23;9(4):E1055-E1062. doi: 10.9778/cmajo.20210091. Print 2021 Oct-Dec.
Several Canadian provinces have introduced reimbursement policies mandating substitution of innovator biologics with lower-cost biosimilars. We estimated the number of patients affected and cost implications if such policy changes were to be implemented in Ontario, Canada.
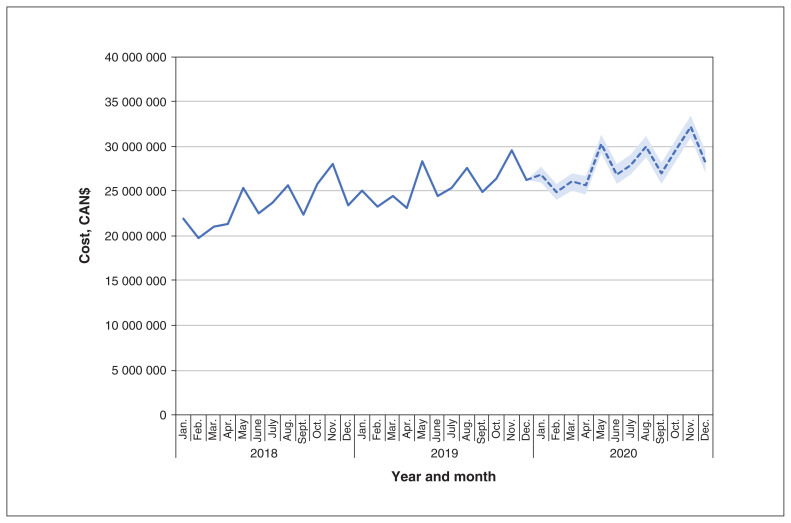
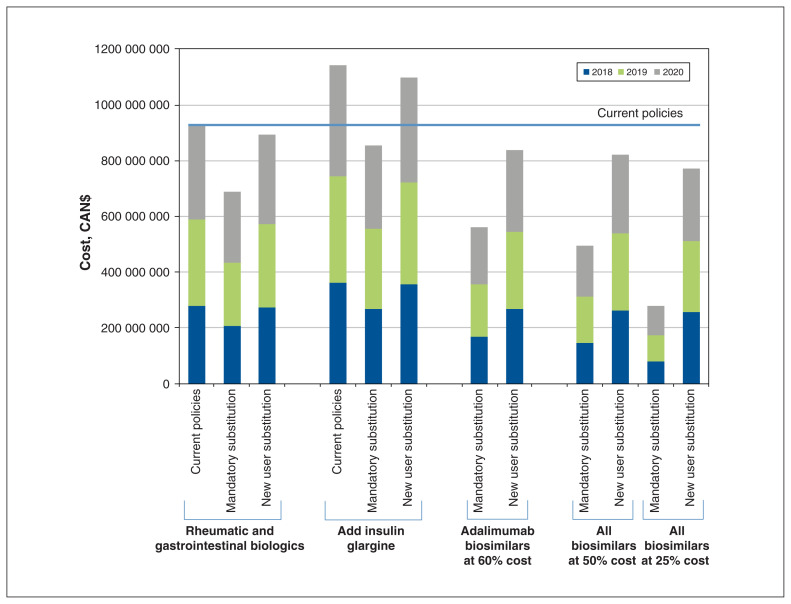
We conducted a cross-sectional time series analysis of Ontarians dispensed publicly funded biologics indicated for inflammatory diseases (rheumatic conditions, inflammatory bowel disease: infliximab, etanercept, adalimumab) between January 2018 and December 2019, and forecasted trends to Dec. 31, 2020. The primary source of data was pharmacy claims data for all biologics reimbursed by the public drug program. We modelled the number of patients affected and government expenditures (in nominal Canadian dollars) of several biosimilar policy options, including mandatory nonmedical biosimilar substitution, substitution in new users, introduction of a biosimilar for adalimumab, and price negotiations. In a secondary analysis, we included insulin glargine.
In 2018, 14 089 individuals were prescribed a publicly funded biologic for inflammatory diseases. A mandatory nonmedical biosimilar substitution would potentially have affected 7209 patients and saved $238.6 million from 2018 to 2020. A new-user substitution would have affected 757 patients and saved $34.2 million. If an adalimumab biosimilar were to become available, 12 928 patients would be affected by a mandatory nonmedical substitution and the 3-year savings would increase to $645.9 million (all biosimilars priced at 25% of innovator biologics). Finally, an expanded nonmedical substitution policy including insulin glargine would affect 115 895 patients and save $288.7 million (not including adalimumab).
Policies designed to curb rising costs of biologics can have substantially different effects on patients and government expenditures. Such analyses warrant careful consideration of the balance between cost savings and effects on patients.
加拿大的几个省份已经出台了报销政策,要求将创新型生物制剂替换为成本更低的生物类似药。我们评估了如果在安大略省实施此类政策变化,将会影响到多少患者以及会产生多少成本。
我们对 2018 年 1 月至 2019 年 12 月期间接受公共资金资助的生物制剂治疗炎症性疾病(风湿性疾病、炎症性肠病:英夫利昔单抗、依那西普、阿达木单抗)的安大略省患者进行了横断面时间序列分析,并预测了截至 2020 年 12 月 31 日的趋势。主要数据来源是公共药物计划报销的所有生物制剂的药房理赔数据。我们对几种生物类似药政策方案的影响患者数量和政府支出(以加元计价)进行了建模,包括强制性非医疗生物类似药替代、新用户替代、阿达木单抗的生物类似药引入以及价格谈判。在二次分析中,我们纳入了甘精胰岛素。
2018 年,有 14089 名患者开了一种用于治疗炎症性疾病的公共资金资助的生物制剂。强制性非医疗生物类似药替代可能会影响 7209 名患者,并在 2018 年至 2020 年期间节省 2.386 亿加元。新用户替代将影响 757 名患者,并节省 3420 万加元。如果阿达木单抗的生物类似药上市,将有 12928 名患者受到强制性非医疗替代的影响,3 年节省额将增加至 6.459 亿加元(所有生物类似药的价格为创新型生物制剂的 25%)。最后,一个包括甘精胰岛素的扩大的非医疗替代政策将影响 115895 名患者,并节省 2.887 亿加元(不包括阿达木单抗)。
旨在控制生物制剂成本上升的政策可能会对患者和政府支出产生截然不同的影响。此类分析需要仔细考虑成本节约与对患者影响之间的平衡。