Chandan Saurabh, Buddam Avanija, Khan Shahab R, Mohan Babu P, Ramai Daryl, Bilal Mohammad, Dhindsa Banreet, Bhogal Neil, Kassab Lena L, Goyal Hemant, Perisetti Abhilash, Facciorusso Antonio, Adler Douglas G
Division of Gastroenterology & Hepatology, CHI Creighton University Medical Center, Omaha, Nebraska, USA (Saurabh Chandan, Avanija Buddam).
Department of Medicine, Brigham & Women's Hospital, Harvard Medical School, Boston, Massachusetts, USA (Shahab R. Khan).
Ann Gastroenterol. 2021 Nov-Dec;34(6):862-871. doi: 10.20524/aog.2021.0661. Epub 2021 Sep 14.
Splanchnic vein thrombosis is a well-recognized local vascular complication of acute pancreatitis (AP), estimated to occur in approximately 15% of patients. While splanchnic vein recanalization occurs spontaneously in approximately one third of patients, severe complications such as bowel ischemia and liver failure have also been reported. At present, there is no consensus on whether patients presenting with AP-associated splanchnic vein thrombosis should receive therapeutic anticoagulation.
We searched multiple databases from inception through December 2020 to collect studies that compared the clinical outcomes of patients with AP and splanchnic vein thrombosis who received therapeutic anticoagulation (AC group) with those who did not (N-AC group). A meta-analysis was performed to calculate the relative risk (RR) of vessel recanalization, bleeding complications, collateral formation and death in the 2 groups.
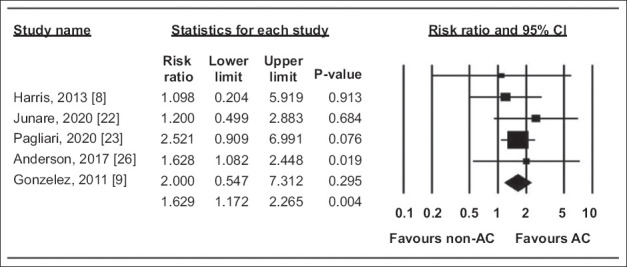
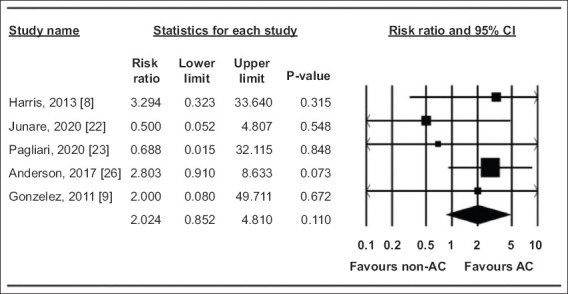
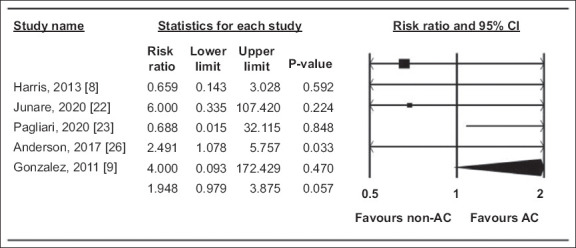
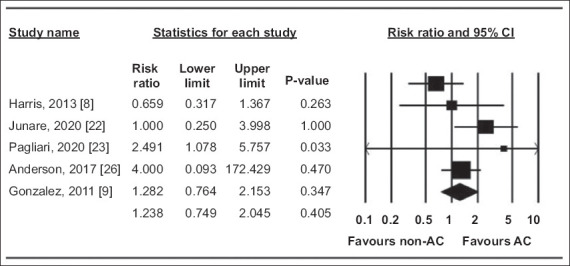
Seven studies with 8353 patients, 339 of whom had splanchnic vein thrombosis, were included in the final analysis. A total of 154 patients (45.4%) had acute severe pancreatitis. A significantly higher proportion of patients had vessel recanalization in the AC group: RR 1.6, 95% confidence interval 1.17-2.27; =0%; P=0.004. There was no difference between the 2 groups in the RR of bleeding complications, collateral formation and death.
Our analysis demonstrated that, among patients with AP-associated splanchnic vein thrombosis, therapeutic anticoagulation resulted in recanalization of the involved vessels without significantly increasing the risk of bleeding complications. There was no difference in the RR of death or the rates of collateral vessel formation during the follow up.
内脏静脉血栓形成是急性胰腺炎(AP)一种公认的局部血管并发症,估计约15%的患者会发生。虽然约三分之一的患者内脏静脉会自发再通,但也有报道出现诸如肠缺血和肝衰竭等严重并发症。目前,对于伴有AP相关性内脏静脉血栓形成的患者是否应接受治疗性抗凝尚无共识。
我们检索了从数据库建立至2020年12月的多个数据库,以收集比较接受治疗性抗凝的AP合并内脏静脉血栓形成患者(抗凝组)与未接受治疗性抗凝的患者(非抗凝组)临床结局的研究。进行荟萃分析以计算两组血管再通、出血并发症、侧支形成和死亡的相对风险(RR)。
最终分析纳入了7项研究,共8353例患者,其中339例有内脏静脉血栓形成。共有154例患者(45.4%)患有急性重症胰腺炎。抗凝组血管再通的患者比例显著更高:RR为1.6,95%置信区间为1.17 - 2.27;I² = 0%;P = 0.004。两组在出血并发症、侧支形成和死亡的RR方面无差异。
我们的分析表明,在伴有AP相关性内脏静脉血栓形成的患者中,治疗性抗凝可使受累血管再通,且不会显著增加出血并发症风险。随访期间死亡的RR及侧支血管形成率无差异。