Huang Allan B, Wu Jenny, Chen Ling, Albright Benjamin B, Previs Rebecca A, Moss Haley A, Davidson Brittany A, Havrilesky Laura J, Melamed Alexander, Wright Jason D
Columbia University Vagelos College of Physicians and Surgeons, United States.
Duke University School of Medicine, United States.
Gynecol Oncol Rep. 2021 Nov 6;38:100887. doi: 10.1016/j.gore.2021.100887. eCollection 2021 Nov.
While primary cytoreductive surgery (PCS) is considered the standard of care for women who present with stage IV endometrial cancer, neoadjuvant chemotherapy (NACT) followed by interval cytoreductive surgery (ICS) has emerged as an alternative treatment strategy. We summarized the literature and compared outcomes of PCS compared to NACT and ICS.
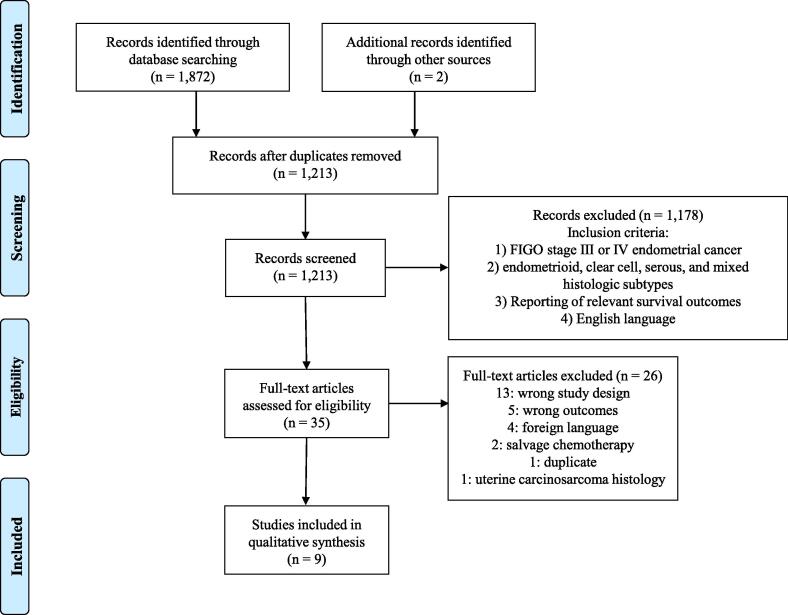
We conducted a systematic search on PubMed, Embase, Web of Science, and Scopus for articles published from January 1, 1990 to December 31, 2020. Key search terms included multiple descriptors of advanced disease status in combination with "endometrial cancer" and "neoadjuvant chemotherapy". Our review included studies that examined survival and surgical outcomes of patients with stage III or IV endometrial cancer treated with neoadjuvant chemotherapy followed by interval cytoreductive surgery versus those who received primary cytoreductive surgery. We excluded studies examining only patients with leiomyosarcomas, carcinosarcomas, and stromal sarcomas due to the biologic heterogeneity of these malignancies.
The nine included studies encompassed 5,844 patients, of which 1,317 (22.5%) received NACT and 4,527 received PCS (77.5%). With the exception of a single study, all were retrospective observational studies or case series. Use of NACT in patients with stage IV EC increased from 16.0% in 2010 to 23.9% in 2015. Five studies analyzed median overall survival and all but one reported no significant difference between NACT + ICS vs. PCS. Optimal cytoreduction (<1 cm of residual disease) rates were similar across both treatment groups in three separate analyses, however pooled data suggest improved rates of optimal cytoreduction for NACT + ICS vs. PCS patients (81.9% vs. 51.5% respectively). Patients receiving NACT experienced significantly shorter hospital admissions and lower operative times compared to PCS counterparts.
NACT followed by ICS reduces perioperative morbidity while offering similar overall survival.
虽然原发性细胞减灭术(PCS)被认为是IV期子宫内膜癌女性患者的标准治疗方法,但新辅助化疗(NACT)后行间隔细胞减灭术(ICS)已成为一种替代治疗策略。我们总结了相关文献,并比较了PCS与NACT和ICS的治疗结果。
我们在PubMed、Embase、Web of Science和Scopus上进行了系统检索,以查找1990年1月1日至2020年12月31日发表的文章。关键检索词包括多种晚期疾病状态描述符与“子宫内膜癌”和“新辅助化疗”的组合。我们的综述纳入了研究新辅助化疗后行间隔细胞减灭术与接受原发性细胞减灭术的III期或IV期子宫内膜癌患者的生存和手术结果的研究。由于这些恶性肿瘤的生物学异质性,我们排除了仅研究平滑肌肉瘤、癌肉瘤和间质肉瘤患者的研究。
纳入的9项研究共涉及5844例患者,其中1317例(22.5%)接受了NACT,4527例接受了PCS(77.5%)。除一项研究外,所有研究均为回顾性观察性研究或病例系列。IV期子宫内膜癌患者中NACT的使用比例从2010年的16.0%增至2015年的23.9%。五项研究分析了中位总生存期,但除一项研究外,其他所有研究均报告NACT+ICS与PCS之间无显著差异。在三项独立分析中,两个治疗组的最佳细胞减灭(残留病灶<1cm)率相似,但汇总数据表明,NACT+ICS组患者的最佳细胞减灭率高于PCS组患者(分别为81.9%和51.5%)。与接受PCS的患者相比,接受NACT的患者住院时间明显缩短,手术时间也更短。
NACT后行ICS可降低围手术期发病率,同时提供相似的总生存期。