The European Reference Network for Rare, Low Prevalence and Complex Diseases of the Heart-ERN GUARD-Heart, Department of Pediatric Cardiology and Cardiac Surgery, Heart and Lung Transplantation, Bambino Gesù Children Hospital and Research Institute, IRCCS, 00165 Rome, Italy.
Laboratory of Medical Genetics, Translational Cytogenomics Research Unit, Bambino Gesù Children Hospital and Research Institute, IRCCS, 00165 Rome, Italy.
Biomolecules. 2021 Oct 25;11(11):1578. doi: 10.3390/biom11111578.
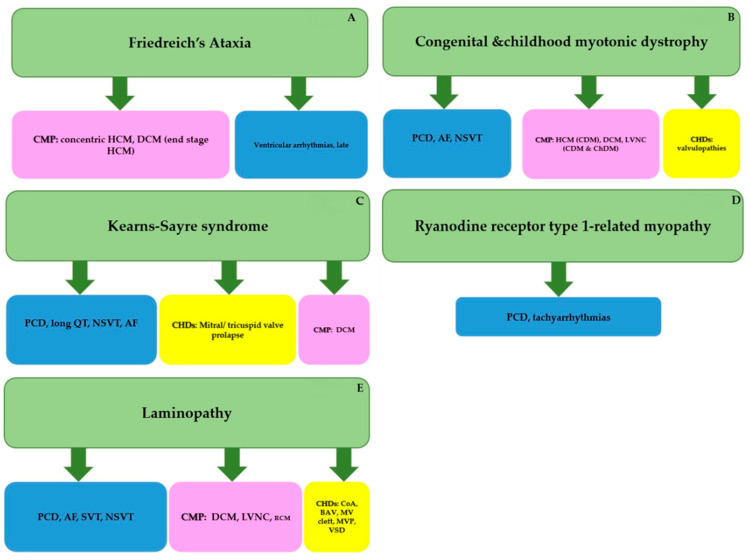
Neuromuscular disorders (NMDs) are highly heterogenous from both an etiological and clinical point of view. Their signs and symptoms are often multisystemic, with frequent cardiac involvement. In fact, childhood onset forms can predispose a person to various progressive cardiac abnormalities including cardiomyopathies (CMPs), valvulopathies, atrioventricular conduction defects (AVCD), supraventricular tachycardia (SVT) and ventricular arrhythmias (VA). In this review, we selected and described five specific NMDs: Friedreich's Ataxia (FRDA), congenital and childhood forms of Myotonic Dystrophy type 1 (DM1), Kearns Sayre Syndrome (KSS), Ryanodine receptor type 1-related myopathies (-RM) and Laminopathies. These changes are widely investigated in adults but less researched in children. We focused on these specific topics due their relative frequency and their potential unexpected cardiac manifestations in children. Moreover these conditions present different inheritance patterns and mechanisms of action. We decided not to discuss Duchenne and Becker muscular dystrophies due to extensive work regarding the cardiac aspects in children. For each described NMD, we focused on the possible cardiac manifestations such as different types of CMPs (dilated-DCM, hypertrophic-HCM, restrictive-RCM or left ventricular non compaction-LVNC), structural heart abnormalities (including valvulopathies), and progressive heart rhythm changes (AVCD, SVT, VA). We describe the current management strategies for these conditions. We underline the importance, especially for children, of a serial multidisciplinary personalized approach and the need for periodic surveillance by a dedicated heart team. This is largely due to the fact that in children, the diagnosis of certain NMDs might be overlooked and the cardiac aspect can provide signs of their presence even prior to overt neurological diagnosis.
神经肌肉疾病(NMDs)从病因学和临床角度来看都具有高度异质性。它们的体征和症状通常是多系统的,常伴有心脏受累。事实上,儿童发病形式可能使人易患各种进行性心脏异常,包括心肌病(CMPs)、瓣膜病、房室传导障碍(AVCD)、室上性心动过速(SVT)和室性心律失常(VA)。在这篇综述中,我们选择并描述了五种特定的 NMD:弗里德里希共济失调(FRDA)、先天性和儿童型 1 型肌强直性营养不良(DM1)、Kearns-Sayre 综合征(KSS)、兰尼碱受体 1 型相关肌病(-RM)和层粘连蛋白病。这些变化在成人中得到了广泛研究,但在儿童中研究较少。我们关注这些特定主题是因为它们的相对频率及其在儿童中潜在的意外心脏表现。此外,这些疾病具有不同的遗传模式和作用机制。我们决定不讨论杜氏肌营养不良症和贝克肌营养不良症,因为已经有大量关于儿童心脏方面的工作。对于每种描述的 NMD,我们都关注可能的心脏表现,如不同类型的 CMP(扩张型-DCM、肥厚型-HCM、限制型-RCM 或左心室非致密化-LVNC)、结构性心脏异常(包括瓣膜病)和进行性心律变化(AVCD、SVT、VA)。我们描述了这些疾病的当前管理策略。我们强调了特别是对于儿童,采用连续的多学科个性化方法的重要性,以及需要由专门的心脏团队进行定期监测。这主要是因为在儿童中,某些 NMD 的诊断可能被忽视,而心脏方面甚至可以在明显的神经诊断之前提供其存在的迹象。