Miclea Diana, Alkhzouz Camelia, Bucerzan Simona, Grigorescu-Sido Paula, Popp Radu Anghel, Pascanu Ionela Maria, Cret Victoria, Ghervan Cristina, Blaga Ligia, Zaharie Gabriela
Molecular Sciences Department, "Iuliu Hatieganu" University of Medicine and Pharmacy, 400012 Cluj-Napoca, Romania.
Medical Genetics Department, Clinical Emergency Hospital for Children, 400370 Cluj-Napoca, Romania.
Diagnostics (Basel). 2021 Nov 14;11(11):2107. doi: 10.3390/diagnostics11112107.
Differences in sex development (DSD) are often correlated with a genetic etiology. This study aimed to assess the etiology of DSD patients following a protocol of genetic testing.
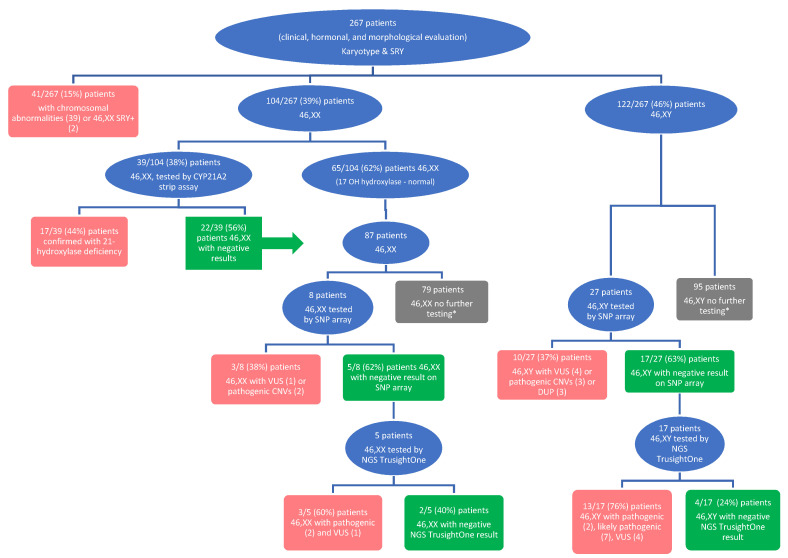
This study prospectively investigated a total of 267 patients with DSD who presented to Clinical Emergency Hospital for Children Cluj-Napoca between January 2012 and December 2019. Each patient was clinically, biochemically, and morphologically evaluated. As a first intervention, the genetic test included karyotype + testing. A high value of 17-hydroxyprogesterone was found in 39 patients, in whom strip assay analysis of the gene was subsequently performed. A total of 35 patients were evaluated by chromosomal microarray technique, and 22 patients were evaluated by the NGS of a gene panel.
The karyotype analysis established the diagnosis in 15% of the patients, most of whom presented with sex chromosome abnormalities. Genetic testing of established a confirmation of the diagnosis in 44% of patients tested. SNP array analysis was particularly useful in patients with syndromic DSD; 20% of patients tested presented with pathogenic CNVs or uniparental disomy. Gene panel sequencing established the diagnosis in 11 of the 22 tested patients (50%), and the androgen receptor gene was most often involved in these patients. The genes that presented as pathogenic or likely pathogenic variants or variants of uncertain significance were , , , , , , , , , , , , , and genes.
An evaluation following a genetic testing protocol that included karyotype and gene testing, analysis, chromosomal analysis by microarray, and high-throughput sequencing were useful in establishing the diagnosis, with a spectrum of diagnostic yield depending on the technique (between 15 and 50%). Additionally, new genetic variants not previously described in DSD were observed.
性发育差异(DSD)通常与遗传病因相关。本研究旨在按照基因检测方案评估DSD患者的病因。
本研究前瞻性地调查了2012年1月至2019年12月期间在克卢日 - 纳波卡市儿童临床急诊医院就诊的267例DSD患者。对每位患者进行了临床、生化和形态学评估。作为首要干预措施,基因检测包括核型分析 + 检测。在39例患者中发现17 - 羟孕酮值升高,随后对这些患者进行了基因的条带分析检测。共35例患者通过染色体微阵列技术进行评估,22例患者通过基因panel的二代测序进行评估。
核型分析在15%的患者中确立了诊断,其中大多数患者存在性染色体异常。基因检测在44%的检测患者中证实了诊断。SNP阵列分析在综合征性DSD患者中特别有用;20%的检测患者存在致病性拷贝数变异或单亲二倍体。基因panel测序在22例检测患者中的11例(50%)中确立了诊断,这些患者中雄激素受体基因最常受累。呈现为致病性或可能致病性变异或意义未明变异的基因有、、、、、、、、、、、、、和基因。
按照包括核型和基因检测、分析、微阵列染色体分析以及高通量测序的基因检测方案进行评估,有助于确立诊断,诊断率因技术不同而有所差异(在15%至50%之间)。此外,还观察到了DSD中先前未描述的新的基因变异。