Jimeno-Almazán Amaya, Pallarés Jesús G, Buendía-Romero Ángel, Martínez-Cava Alejandro, Courel-Ibáñez Javier
Department of Infectious Diseases, Hospital Universitario Santa Lucía, Cartagena, 30202 Murcia, Spain.
Human Performance & Sport Sciences Laboratory, University of Murcia, 30720 Murcia, Spain.
J Clin Med. 2021 Nov 20;10(22):5434. doi: 10.3390/jcm10225434.
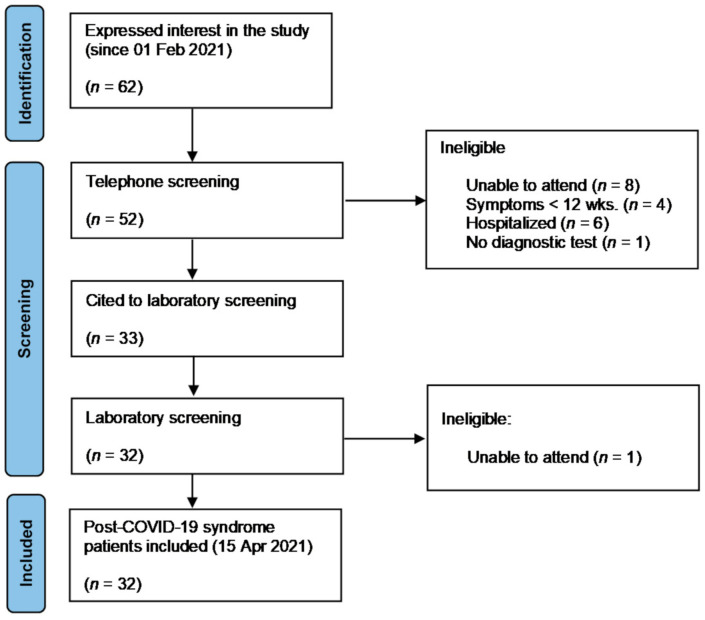
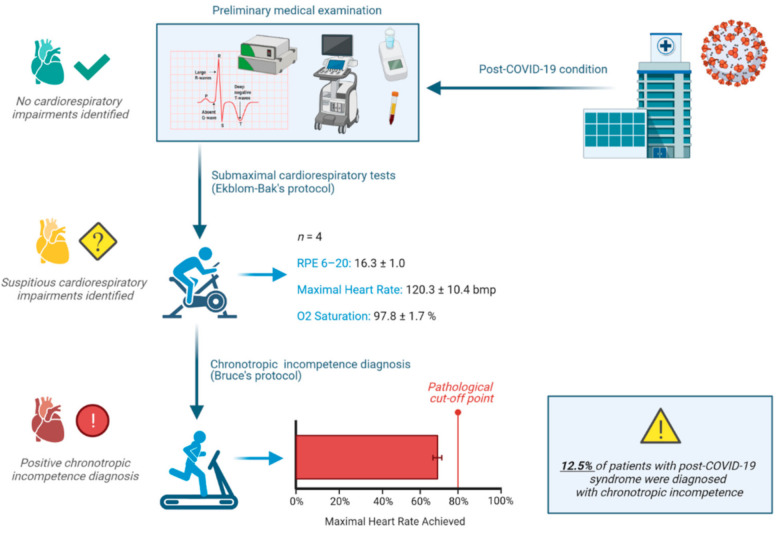
Patients recovering from COVID-19 commonly report persistence of dyspnea, exertional fatigue, and difficulties in carrying out their daily activities. However, the nature of these symptoms is still unknown. The purpose of the study was to identify limiting causes of cardiopulmonary origin for the performance of physical exercise in post-COVID-19 condition that could explain the symptomatic persistence of dyspnea or fatigue-related symptoms. Thirty-two non-hospitalized patients with post-COVID-19 condition (i.e., still presenting a chronic symptomatic phase lasting >90 days since debut of symptoms that lasted for at least 2 months and cannot be explained by an alternative diagnosis) completed a clinical examination including echocardiography, submaximal and maximal cardiorespiratory fitness tests (Ekblom-Bak and Bruce's protocols), and a battery of validated questionnaires about fatigue and exercise intolerance. Four participants (12.5%) reported an abnormal cardiac response to exercise during the submaximal test, which aroused suspicion of the presence of chronotropic incompetence. All of them were confirmed with a positive diagnosis maximal exercise test after cardiology screening, even with a comprehensive clinical examination, resting ECG, and echocardiogram, without other findings. No statistical differences were found in any physiological variables or questionnaire values, between patients with positive and negative diagnoses. Chronotropic incompetence and other autonomic disorders may appear in patients with mild forms of COVID-19 presentation and may persist in the long term, being responsible for exercise intolerance after resolution of acute infection. Clinicians should be aware that chronotropic incompetence and other autonomic disorders may be a complication of COVID-19 and should consider appropriate diagnostic and therapeutic interventions in these patients, especially when early exercise-related fatigability is reported.
从新冠病毒感染中康复的患者普遍报告存在呼吸困难、运动性疲劳以及进行日常活动困难的情况。然而,这些症状的本质仍不明确。本研究的目的是确定新冠康复后状态下影响体育锻炼表现的心肺源性限制因素,这些因素可能解释呼吸困难或疲劳相关症状的持续存在。32名非住院的新冠康复患者(即仍处于慢性症状期,自症状首次出现起持续超过90天,症状持续至少2个月且无法用其他诊断解释)完成了一项临床检查,包括超声心动图、次极量和极量心肺适能测试(埃克布隆 - 巴克和布鲁斯方案),以及一系列关于疲劳和运动不耐受的有效问卷。4名参与者(12.5%)在次极量测试中报告运动时心脏反应异常,这引发了对变时性功能不全存在的怀疑。经心脏病学筛查后,通过极量运动测试均确诊为阳性,即便进行了全面的临床检查、静息心电图和超声心动图检查,也未发现其他异常。阳性和阴性诊断的患者在任何生理变量或问卷值方面均未发现统计学差异。变时性功能不全和其他自主神经紊乱可能出现在轻症新冠患者中,并可能长期持续存在,导致急性感染消退后出现运动不耐受。临床医生应意识到变时性功能不全和其他自主神经紊乱可能是新冠的并发症,对于这些患者应考虑适当的诊断和治疗干预措施,尤其是当患者报告早期运动相关疲劳时。