Li Jie, Scott J Brady, Fink James B, Reed Brooke, Roca Oriol, Dhand Rajiv
Division of Respiratory Care, Department of Cardiopulmonary Sciences, Rush University, 600 S Paulina St, Suite 765, Chicago, IL, 60612, USA.
Aerogen Pharma Corp, San Mateo, CA, USA.
Ann Intensive Care. 2021 Nov 27;11(1):164. doi: 10.1186/s13613-021-00949-8.
Optimal flow settings during high-flow nasal cannula (HFNC) therapy are unknown. We investigated the optimal flow settings during HFNC therapy based on breathing pattern and tidal inspiratory flows in patients with acute hypoxemic respiratory failure (AHRF).
We conducted a prospective clinical study in adult hypoxemic patients treated by HFNC with a fraction of inspired oxygen (FO) ≥ 0.4. Patient's peak tidal inspiratory flow (PTIF) was measured and HFNC flows were set to match individual PTIF and then increased by 10 L/min every 5-10 min up to 60 L/min. FO was titrated to maintain pulse oximetry (SpO) of 90-97%. SpO/FO, respiratory rate (RR), ROX index [(SpO/FO)/RR], and patient comfort were recorded after 5-10 min on each setting. We also conducted an in vitro study to explore the relationship between the HFNC flows and the tracheal FO, peak inspiratory and expiratory pressures.
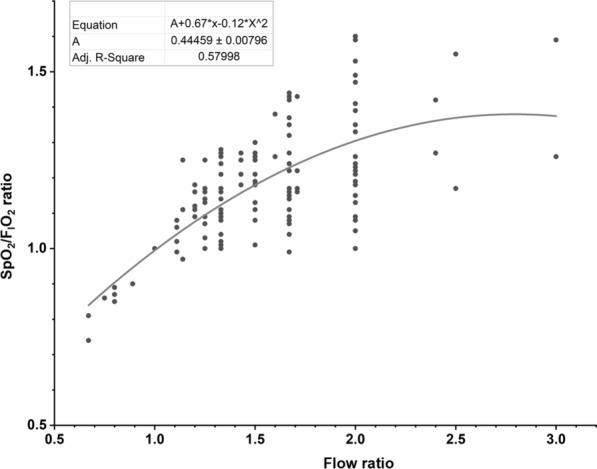
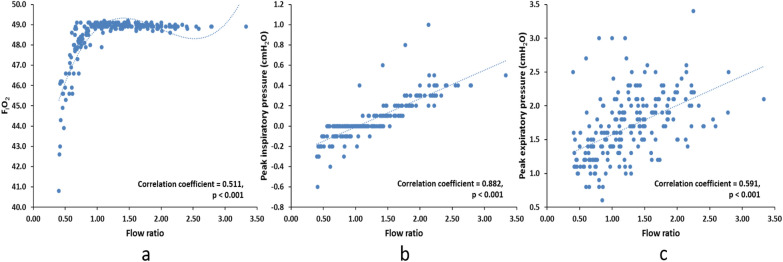
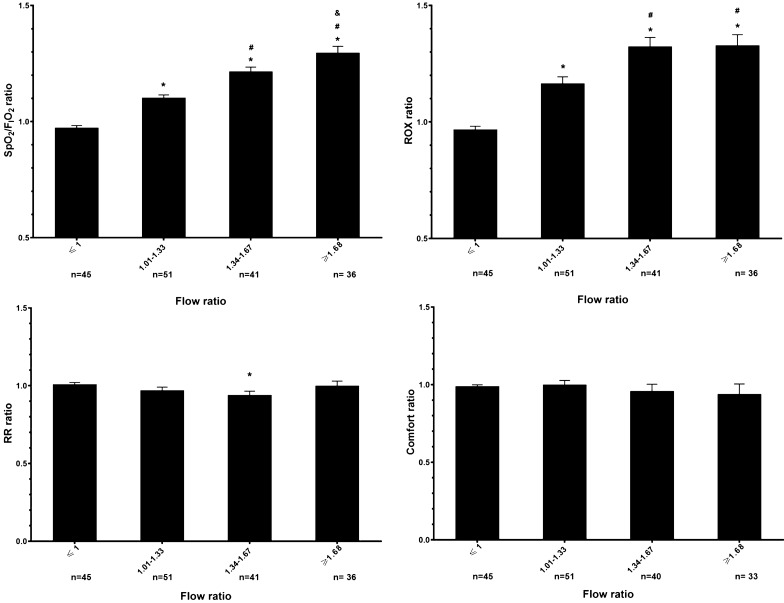
Forty-nine patients aged 58.0 (SD 14.1) years were enrolled. At enrollment, HFNC flow was set at 45 (38, 50) L/min, with an FO at 0.62 (0.16) to obtain an SpO/FO of 160 (40). Mean PTIF was 34 (9) L/min. An increase in HFNC flows up to two times of the individual patient's PTIF, incrementally improved oxygenation but the ROX index plateaued with HFNC flows of 1.34-1.67 times the individual PTIF. In the in vitro study, when the HFNC flow was set higher than PTIF, tracheal peak inspiratory and expiratory pressures increased as HFNC flow increased but the FO did not change.
Mean PTIF values in most patients with AHRF were between 30 and 40 L/min. We observed improvement in oxygenation with HFNC flows set above patient PTIF. Thus, a pragmatic approach to set optimal flows in patients with AHRF would be to initiate HFNC flow at 40 L/min and titrate the flow based on improvement in ROX index and patient tolerance.
ClinicalTrials.gov (NCT03738345). Registered on November 13th, 2018. https://clinicaltrials.gov/ct2/show/NCT03738345?term=NCT03738345&draw=2&rank=1.
高流量鼻导管(HFNC)治疗期间的最佳流量设置尚不清楚。我们基于急性低氧性呼吸衰竭(AHRF)患者的呼吸模式和吸气潮气量,研究了HFNC治疗期间的最佳流量设置。
我们对接受HFNC治疗且吸入氧分数(FO)≥0.4的成年低氧血症患者进行了一项前瞻性临床研究。测量患者的吸气潮气量峰值(PTIF),将HFNC流量设置为与个体PTIF相匹配,然后每5 - 10分钟增加10 L/min,直至60 L/min。滴定FO以维持脉搏血氧饱和度(SpO)在90 - 97%。在每个设置下5 - 10分钟后记录SpO/FO、呼吸频率(RR)、ROX指数[(SpO/FO)/RR]和患者舒适度。我们还进行了一项体外研究,以探讨HFNC流量与气管FO、吸气和呼气峰值压力之间的关系。
纳入了49例年龄为58.0(标准差±14.1)岁的患者。入组时,HFNC流量设置为45(38,50)L/min,FO为0.62(0.16),以获得SpO/FO为160(40)。平均PTIF为34(9)L/min。将HFNC流量增加至个体患者PTIF的两倍,可逐渐改善氧合,但当HFNC流量为个体PTIF的1.34 - 1.67倍时,ROX指数趋于平稳。在体外研究中,当HFNC流量设置高于PTIF时,气管吸气和呼气峰值压力随HFNC流量增加而升高,但FO不变。
大多数AHRF患者的平均PTIF值在30至40 L/min之间。我们观察到将HFNC流量设置高于患者PTIF时氧合得到改善。因此,为AHRF患者设置最佳流量的实用方法是起始HFNC流量为40 L/min,并根据ROX指数的改善和患者耐受性滴定流量。
ClinicalTrials.gov(NCT03738345)。于2018年11月13日注册。https://clinicaltrials.gov/ct2/show/NCT03738345?term=NCT03738345&draw=2&rank=1。