Division of Oncology, Department of Medicine, Washington University School of Medicine in St. Louis, St. Louis, MO 63110.
Siteman Cancer Center, Washington University School of Medicine in St. Louis, St. Louis, MO 63110.
Proc Natl Acad Sci U S A. 2021 Dec 7;118(49). doi: 10.1073/pnas.2116427118.
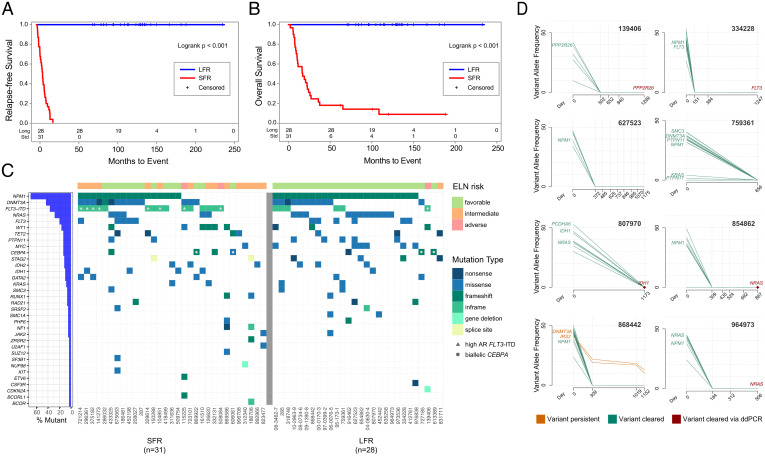
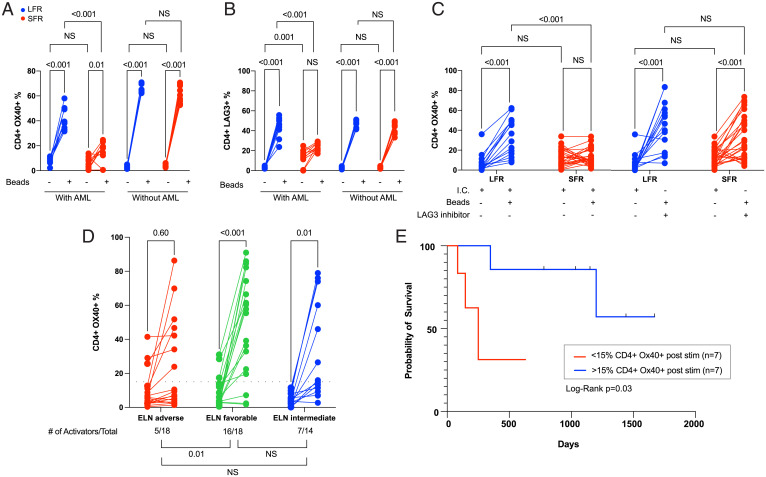
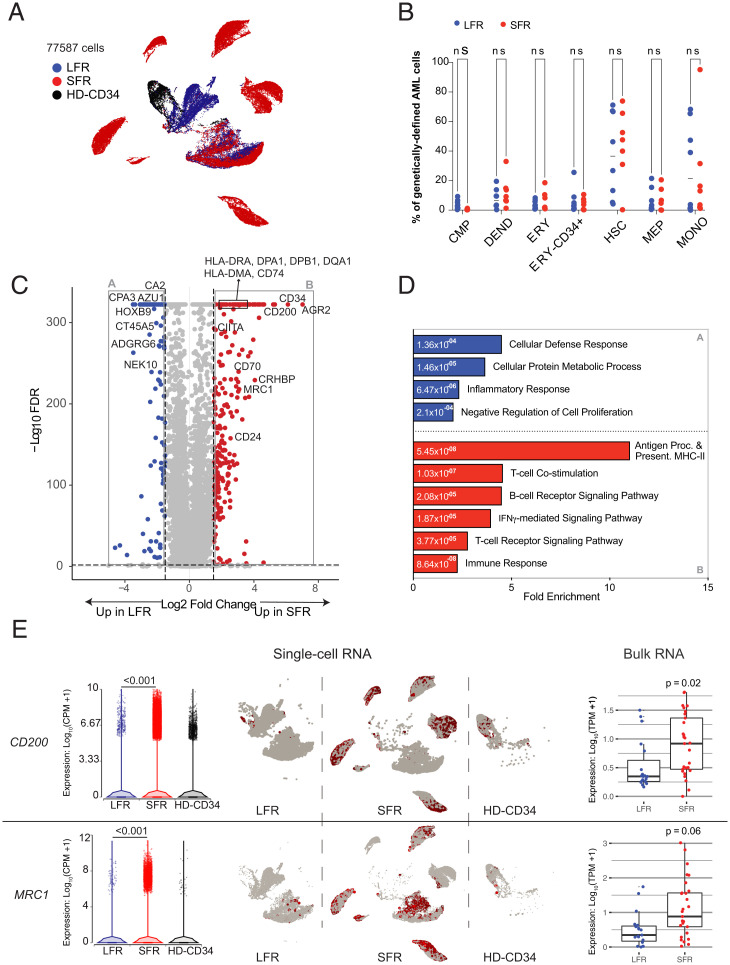
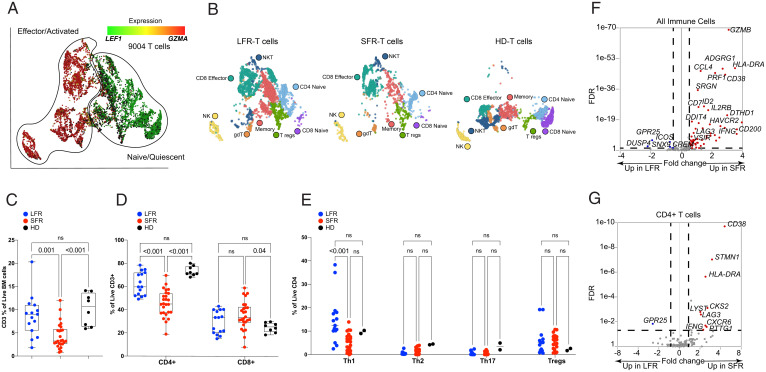
Acute myeloid leukemia (AML) patients rarely have long first remissions (LFRs; >5 y) after standard-of-care chemotherapy, unless classified as favorable risk at presentation. Identification of the mechanisms responsible for long vs. more typical, standard remissions may help to define prognostic determinants for chemotherapy responses. Using exome sequencing, RNA-sequencing, and functional immunologic studies, we characterized 28 normal karyotype (NK)-AML patients with >5 y first remissions after chemotherapy (LFRs) and compared them to a well-matched group of 31 NK-AML patients who relapsed within 2 y (standard first remissions [SFRs]). Our combined analyses indicated that genetic-risk profiling at presentation (as defined by European LeukemiaNet [ELN] 2017 criteria) was not sufficient to explain the outcomes of many SFR cases. Single-cell RNA-sequencing studies of 15 AML samples showed that SFR AML cells differentially expressed many genes associated with immune suppression. The bone marrow of SFR cases had significantly fewer CD4 Th1 cells; these T cells expressed an exhaustion signature and were resistant to activation by T cell receptor stimulation in the presence of autologous AML cells. T cell activation could be restored by removing the AML cells or blocking the inhibitory major histocompatibility complex class II receptor, LAG3. Most LFR cases did not display these features, suggesting that their AML cells were not as immunosuppressive. These findings were confirmed and extended in an independent set of 50 AML cases representing all ELN 2017 risk groups. AML cell-mediated suppression of CD4 T cell activation at presentation is strongly associated with unfavorable outcomes in AML patients treated with standard chemotherapy.
急性髓系白血病(AML)患者在接受标准化疗后很少有长首次缓解期(LFR;>5 年),除非在初诊时被归类为低危。确定导致长缓解期与更典型的标准缓解期的机制可能有助于确定化疗反应的预后决定因素。我们通过外显子组测序、RNA 测序和功能免疫研究,对 28 例化疗后首次缓解期>5 年的核型正常(NK)-AML 患者(LFR)进行了特征描述,并将其与 31 例 2 年内复发的核型正常(NK)-AML 患者(标准首次缓解期[SFR])进行了比较。我们的综合分析表明,初诊时的遗传风险分析(根据欧洲白血病网络[ELN]2017 标准定义)不足以解释许多 SFR 病例的结果。对 15 例 AML 样本的单细胞 RNA 测序研究表明,SFR AML 细胞差异表达了许多与免疫抑制相关的基因。SFR 病例的骨髓中 CD4 Th1 细胞明显减少;这些 T 细胞表达了衰竭特征,并且在存在自体 AML 细胞的情况下,对抗原受体刺激的激活具有抗性。通过去除 AML 细胞或阻断抑制性主要组织相容性复合体 II 受体 LAG3,可以恢复 T 细胞的激活。大多数 LFR 病例没有表现出这些特征,这表明它们的 AML 细胞没有那么具有免疫抑制性。这些发现在一组代表所有 ELN 2017 风险组的 50 例 AML 病例中得到了证实和扩展。AML 细胞在初次发病时对 CD4 T 细胞激活的抑制与接受标准化疗的 AML 患者的不良预后密切相关。